Blake E S Taylor, Smit Patel, Patrick Hilden, Fadar Oliver Otite, Kiwon Lee, Gaurav Gupta, Priyank Khandelwal
{"title":"The weekend effect on mechanical thrombectomy: A nationwide analysis before and after the pivotal 2015 trials.","authors":"Blake E S Taylor, Smit Patel, Patrick Hilden, Fadar Oliver Otite, Kiwon Lee, Gaurav Gupta, Priyank Khandelwal","doi":"10.4103/bc.bc_23_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>As hospitals rapidly implement mechanical thrombectomy (MT) into stroke protocols following the pivotal trials in 2015, access to and outcomes from MT may be poorer for weekend-admitted patients. We sought to investigate whether a \"weekend effect\" influences MT outcomes nationally.</p><p><strong>Materials and methods: </strong>We identified stroke patients from 2010-2014 (pre-trials) to 2015-2017 (posttrials) using the Nationwide Readmissions Database. On multivariate analyses, we determined factors independently associated with receiving MT. Among MT patients, we then determined whether weekend admission was independently associated with inpatient mortality and unfavorable discharge.</p><p><strong>Results: </strong>We identified 2,121,462 patients from 2010 to 2014, of whom 1.11% of weekday-admitted and 1.08% of weekend-admitted patients underwent MT. Of the 1,286,501 patients identified from 2015 to 2017, MT was performed in 2.82% and 2.91%, respectively. In the earlier cohort, weekend admission was independently associated with reduced odds of MT (odds ratio [OR] = 0.92, 95% confidence interval [CI]: 0.89-0.95, <i>P</i> < 0.0001), although this was not statistically significant in the later cohort. During both periods, age >80 years was independently associated with a reduced likelihood of receiving MT, and status as a teaching or large bed-size hospital was associated with a greater likelihood. Weekend admission was independently associated with unfavorable discharge only in the 2015-2017 cohort (OR = 1.11, 95% CI: 1.02-1.22, <i>P</i> = 0.02).</p><p><strong>Conclusions: </strong>While nationwide access to MT has improved for weekend-admitted patients, the elderly and those at smaller, nonteaching hospitals remain underserved. Although we found no effect of weekend admission on inpatient mortality, since the major shift in practice, an emerging \"weekend effect\" may influence discharge outcomes. Data suggest that some hospitals are being challenged to provide this new standard of care efficiently and equitably.</p>","PeriodicalId":9288,"journal":{"name":"Brain Circulation","volume":"8 3","pages":"137-145"},"PeriodicalIF":4.8000,"publicationDate":"2022-09-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/41/c9/BC-8-137.PMC9578310.pdf","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain Circulation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/bc.bc_23_22","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 4
Abstract
Objectives: As hospitals rapidly implement mechanical thrombectomy (MT) into stroke protocols following the pivotal trials in 2015, access to and outcomes from MT may be poorer for weekend-admitted patients. We sought to investigate whether a "weekend effect" influences MT outcomes nationally.
Materials and methods: We identified stroke patients from 2010-2014 (pre-trials) to 2015-2017 (posttrials) using the Nationwide Readmissions Database. On multivariate analyses, we determined factors independently associated with receiving MT. Among MT patients, we then determined whether weekend admission was independently associated with inpatient mortality and unfavorable discharge.
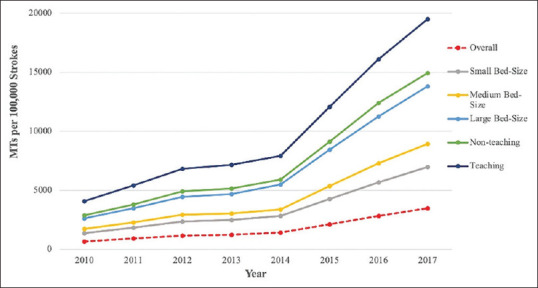
Results: We identified 2,121,462 patients from 2010 to 2014, of whom 1.11% of weekday-admitted and 1.08% of weekend-admitted patients underwent MT. Of the 1,286,501 patients identified from 2015 to 2017, MT was performed in 2.82% and 2.91%, respectively. In the earlier cohort, weekend admission was independently associated with reduced odds of MT (odds ratio [OR] = 0.92, 95% confidence interval [CI]: 0.89-0.95, P < 0.0001), although this was not statistically significant in the later cohort. During both periods, age >80 years was independently associated with a reduced likelihood of receiving MT, and status as a teaching or large bed-size hospital was associated with a greater likelihood. Weekend admission was independently associated with unfavorable discharge only in the 2015-2017 cohort (OR = 1.11, 95% CI: 1.02-1.22, P = 0.02).
Conclusions: While nationwide access to MT has improved for weekend-admitted patients, the elderly and those at smaller, nonteaching hospitals remain underserved. Although we found no effect of weekend admission on inpatient mortality, since the major shift in practice, an emerging "weekend effect" may influence discharge outcomes. Data suggest that some hospitals are being challenged to provide this new standard of care efficiently and equitably.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
