Long-term outcomes of severe rheumatic mitral stenosis after undergoing percutaneous mitral commissurotomy and mitral valve replacement: A 10-year experience.
{"title":"Long-term outcomes of severe rheumatic mitral stenosis after undergoing percutaneous mitral commissurotomy and mitral valve replacement: A 10-year experience.","authors":"Wasinee Promratpan, Nonthikorn Theerasuwipakorn, Vorarit Lertsuwunseri, Suphot Srimahachota","doi":"10.34172/jcvtr.2022.16","DOIUrl":null,"url":null,"abstract":"<p><p><b><i>Introduction:</i></b> Percutaneous mitral commissurotomy (PTMC) and mitral valve replacement (MVR) are treatments of choice for severe rheumatic mitral stenosis (MS). Data regarding the long-term outcomes of patients who underwent PTMC and MVR are limited. <b><i>Methods:</i></b> A retrospective cohort study was conducted to evaluate the long-term outcomes of patients with severe rheumatic MS who underwent PTMC or MVR between 2010 to 2020. The primary outcome comprised of all-cause death, stroke or systemic embolism, heart failure hospitalization and re-intervention. Cox regression was used to investigate predictors of the primary outcome. <b><i>Results:</i></b> 264 patients were included in analysis, 164 patients (62.1%) in PTMC group and 100 patients in MVR group (37.9%). The majority were females (80.7%) and had atrial fibrillation (68.6%). The mean age was 49.52 (SD: 13.03) years old. MVR group had more age and AF, higher Wilkins' score with smaller MVA. Primary outcome occurred significantly higher in PTMC group (37.2% vs 22%, <i>P</i>=0.002), as well as, re-intervention (18.3% vs 0%, <i>P</i><0.001). However, all-cause mortality, stroke or systemic embolism and heart failure hospitalization were not significantly different. In multivariate Cox regression analysis, PTMC (HR 1.94; 95%CI 1.14, 3.32; <i>P</i>=0.015), older age (HR 1.03; 95%CI 1.01, 1.06; <i>P</i>=0.009) and SPAP > 50 mmHg (HR 2.99; 95%CI 1.01, 8.84; <i>P</i>=0.047) were the only predictors of primary outcome. <b><i>Conclusion:</i></b> Primary outcome occurred in PTMC group more than MVR group which was driven by re-intervention. However, all-cause mortality, stroke or systemic embolism and heart failure hospitalization were not significantly different.</p>","PeriodicalId":15207,"journal":{"name":"Journal of Cardiovascular and Thoracic Research","volume":"14 2","pages":"101-107"},"PeriodicalIF":0.7000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9339733/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular and Thoracic Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34172/jcvtr.2022.16","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/6/12 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
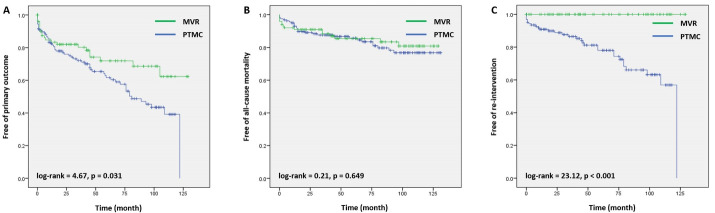
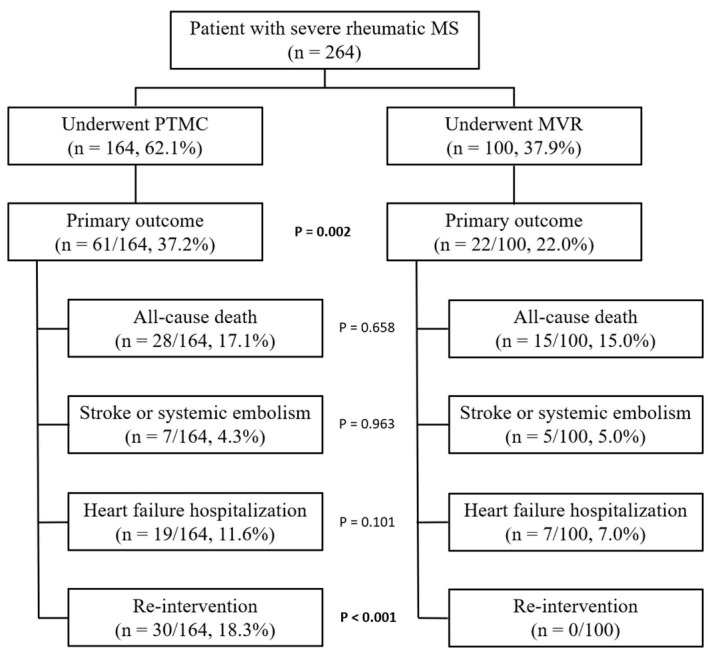
Introduction: Percutaneous mitral commissurotomy (PTMC) and mitral valve replacement (MVR) are treatments of choice for severe rheumatic mitral stenosis (MS). Data regarding the long-term outcomes of patients who underwent PTMC and MVR are limited. Methods: A retrospective cohort study was conducted to evaluate the long-term outcomes of patients with severe rheumatic MS who underwent PTMC or MVR between 2010 to 2020. The primary outcome comprised of all-cause death, stroke or systemic embolism, heart failure hospitalization and re-intervention. Cox regression was used to investigate predictors of the primary outcome. Results: 264 patients were included in analysis, 164 patients (62.1%) in PTMC group and 100 patients in MVR group (37.9%). The majority were females (80.7%) and had atrial fibrillation (68.6%). The mean age was 49.52 (SD: 13.03) years old. MVR group had more age and AF, higher Wilkins' score with smaller MVA. Primary outcome occurred significantly higher in PTMC group (37.2% vs 22%, P=0.002), as well as, re-intervention (18.3% vs 0%, P<0.001). However, all-cause mortality, stroke or systemic embolism and heart failure hospitalization were not significantly different. In multivariate Cox regression analysis, PTMC (HR 1.94; 95%CI 1.14, 3.32; P=0.015), older age (HR 1.03; 95%CI 1.01, 1.06; P=0.009) and SPAP > 50 mmHg (HR 2.99; 95%CI 1.01, 8.84; P=0.047) were the only predictors of primary outcome. Conclusion: Primary outcome occurred in PTMC group more than MVR group which was driven by re-intervention. However, all-cause mortality, stroke or systemic embolism and heart failure hospitalization were not significantly different.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
