{"title":"Pemphigoid gestationis and preeclampsia in a donor-egg IVF pregnancy.","authors":"Timothy L Cowan, Mani Makhija, Dedee F Murrell","doi":"10.1097/JW9.0000000000000026","DOIUrl":null,"url":null,"abstract":"Dear Editors, A 47-year-old Caucasian female underwent her second invitro fertilisation pregnancy with the same unrelated egg donor aged 29 and same father aged 44. Early in her pregnancy, she developed pregnancy-induced subclinical hypothyroidism with negative thyroid autoantibodies, normal T4, and a thyroid-stimulating hormone of 2.7, which is elevated compared with the normal range in the first trimester of pregnancy and was commenced on levothyroxine. In the second trimester of this pregnancy, she developed intensely pruritic erythematous patches on her chest (Fig. 1A), which then spread to her trunk and limbs, but spared her peri-umbilical region without obvious blistering. She was referred for investigation of her worsening pruritus despite regular antihistamines and topical steroids. A lesional skin biopsy, stained with hematoxylin and eosin, revealed eosinophils, neutrophils, and edema in the papillary dermis and perivascular inflammation (Fig. 2). On direct immunofluorescence of perilesional skin, there was discontinuous n-serrated linear deposition of complement (C3) at the dermoepidermal junction. Bullous pemphigoid (BP) 180 antibodies were positive with a titer of 3.11 on serum enzymelinked immunosorbent assay, with negative BP230 antibodies. Pemphigoid gestationis (PG) was diagnosed rather than polymorphic eruption of pregnancy due to her positive direct immunofluorescence and BP180 antibodies. During follow-up, consultation to explain her diagnosis of PG, facial and peripheral edema was noted, and preeclampsia was considered. Her blood pressure was 162/95 with proteinuria, and so she was urgently admitted to the hospital. She had been closely monitored during her pregnancy due to her high-risk status from advanced maternal age, and this was the first evidence of preeclampsia during her antenatal care. Therefore, her manifestations of PG commenced approximately 16 weeks before her preeclampsia. There was no personal or family history of hypertension or preeclampsia in the egg donor or father; however, there was a maternal family history of hypertension in her father. For severe preeclampsia, she was managed with labetalol, hydralazine, and intravenous magnesium sulfate but proceeded to have an emergency cesarean at 32 weeks resulting in a male infant with a birth weight of 1.58 kg, Appearance, Pulse, Grimace, Activity and Respiration 5, 7, and 9 at birth, 5 and 10 minutes. He remained in the neonatal intensive care unit and was discharged well at 9 weeks. By 1-week post-delivery, her PG lesions had completely resolved but she had ongoing positive BP180 antibodies at a reducing titer. By 4 weeks post-partum, her hypertension had resolved and anti-hypertensives had ceased. PG is a rare autoimmune disease of pregnancy.1 There has been 1 reported case of PG coinciding with Haemolysis, Elevated Liver enzymes, and Low Platelet count syndrome,2 and a small number of case studies reporting association between PG and preeclampsia.3,4 Donated eggs have been proposed as an allogeneic trigger for PG through the generation of BP180 antibodies from abnormal expression of major histocompatibility complex class II molecules on chorionic villi. This may develop an augmented immune response to the entire fetal genome.5 In this case, the mechanism may underlie hypothyroidism, PG, and preeclampsia. There are no reported cases of a pregnancy complicated by new hypothyroidism, PG, and preeclampsia. This case is unique and may be the first immunogenic link between these 3 diagnoses. This case also highlights the importance of holistic practice within dermatology. In any pregnant woman attending a dermatology clinic with a rash, it is prudent to consider other conditions of pregnancy that may be associated, such as preeclampsia, as in this case.","PeriodicalId":53478,"journal":{"name":"International Journal of Women''s Dermatology","volume":" ","pages":"e026"},"PeriodicalIF":3.1000,"publicationDate":"2022-07-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9276465/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Women''s Dermatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/JW9.0000000000000026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
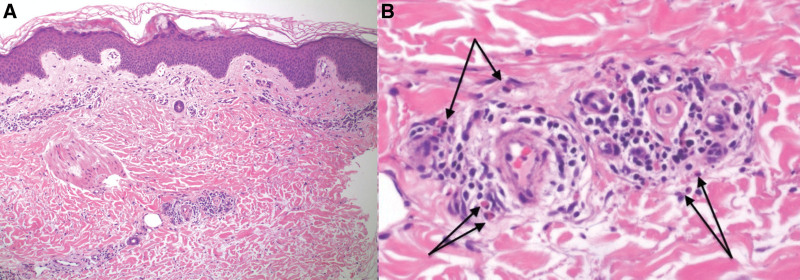
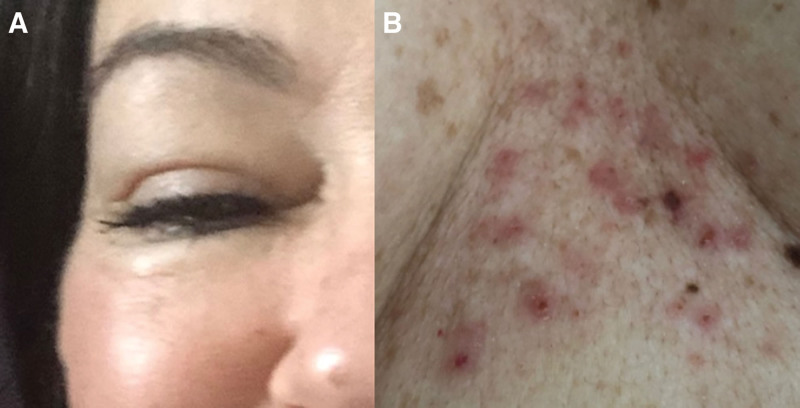
Dear Editors, A 47-year-old Caucasian female underwent her second invitro fertilisation pregnancy with the same unrelated egg donor aged 29 and same father aged 44. Early in her pregnancy, she developed pregnancy-induced subclinical hypothyroidism with negative thyroid autoantibodies, normal T4, and a thyroid-stimulating hormone of 2.7, which is elevated compared with the normal range in the first trimester of pregnancy and was commenced on levothyroxine. In the second trimester of this pregnancy, she developed intensely pruritic erythematous patches on her chest (Fig. 1A), which then spread to her trunk and limbs, but spared her peri-umbilical region without obvious blistering. She was referred for investigation of her worsening pruritus despite regular antihistamines and topical steroids. A lesional skin biopsy, stained with hematoxylin and eosin, revealed eosinophils, neutrophils, and edema in the papillary dermis and perivascular inflammation (Fig. 2). On direct immunofluorescence of perilesional skin, there was discontinuous n-serrated linear deposition of complement (C3) at the dermoepidermal junction. Bullous pemphigoid (BP) 180 antibodies were positive with a titer of 3.11 on serum enzymelinked immunosorbent assay, with negative BP230 antibodies. Pemphigoid gestationis (PG) was diagnosed rather than polymorphic eruption of pregnancy due to her positive direct immunofluorescence and BP180 antibodies. During follow-up, consultation to explain her diagnosis of PG, facial and peripheral edema was noted, and preeclampsia was considered. Her blood pressure was 162/95 with proteinuria, and so she was urgently admitted to the hospital. She had been closely monitored during her pregnancy due to her high-risk status from advanced maternal age, and this was the first evidence of preeclampsia during her antenatal care. Therefore, her manifestations of PG commenced approximately 16 weeks before her preeclampsia. There was no personal or family history of hypertension or preeclampsia in the egg donor or father; however, there was a maternal family history of hypertension in her father. For severe preeclampsia, she was managed with labetalol, hydralazine, and intravenous magnesium sulfate but proceeded to have an emergency cesarean at 32 weeks resulting in a male infant with a birth weight of 1.58 kg, Appearance, Pulse, Grimace, Activity and Respiration 5, 7, and 9 at birth, 5 and 10 minutes. He remained in the neonatal intensive care unit and was discharged well at 9 weeks. By 1-week post-delivery, her PG lesions had completely resolved but she had ongoing positive BP180 antibodies at a reducing titer. By 4 weeks post-partum, her hypertension had resolved and anti-hypertensives had ceased. PG is a rare autoimmune disease of pregnancy.1 There has been 1 reported case of PG coinciding with Haemolysis, Elevated Liver enzymes, and Low Platelet count syndrome,2 and a small number of case studies reporting association between PG and preeclampsia.3,4 Donated eggs have been proposed as an allogeneic trigger for PG through the generation of BP180 antibodies from abnormal expression of major histocompatibility complex class II molecules on chorionic villi. This may develop an augmented immune response to the entire fetal genome.5 In this case, the mechanism may underlie hypothyroidism, PG, and preeclampsia. There are no reported cases of a pregnancy complicated by new hypothyroidism, PG, and preeclampsia. This case is unique and may be the first immunogenic link between these 3 diagnoses. This case also highlights the importance of holistic practice within dermatology. In any pregnant woman attending a dermatology clinic with a rash, it is prudent to consider other conditions of pregnancy that may be associated, such as preeclampsia, as in this case.
期刊介绍:
The IJWD publishes articles pertaining to dermatologic medical, surgical and cosmetic issues faced by female patients and their families. We are interested in original research articles, review articles, unusual case reports, new treatments, clinical trials, education, mentorship and viewpoint articles. Articles dealing with ethical issues in dermatology and medical legal scenarios are also welcome.Very important articles will have accompanying editorials. Topics which our subsections editors look forward to welcoming include: Women’s Health Oncology, Surgery and Aesthetics Pediatric Dermatology Medical Dermatology Society.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
