Olga Lavrynenko, Moulika Baireddy, Srilekha Bodepudi, Hector Santos, James Cortez, Olga Zemlianitsyna, Fernando Sanchez
{"title":"Peritoneal and Pulmonary Tuberculosis in a Postpartum Female with Elevated Cancer Antigen 125 and Ascites.","authors":"Olga Lavrynenko, Moulika Baireddy, Srilekha Bodepudi, Hector Santos, James Cortez, Olga Zemlianitsyna, Fernando Sanchez","doi":"10.1155/2022/7012943","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Peritoneal tuberculosis is a rare form of extrapulmonary tuberculosis and presents a challenging diagnosis because of its nonspecific clinical manifestations. Peritoneal TB mimics other pathologies, including abdominal carcinomatosis, especially when the patient presents with ascites and an elevated cancer antigen (CA)-125 levels. <i>Case Presentation</i>. A postpartum 20-year-old Hispanic female recently discharged after transverse cesarean surgery, presented to the ER with fever, chills, edema, abdominal distension, nausea, and vomiting. The patient was febrile, tachycardic, and hypotensive. Chest X-ray demonstrated alveolar and interstitial consolidations; chest CT revealed tree-in-bud opacities in the right lower lobe, suggestive of atypical (TB)/fungal infection. CT of the abdomen and pelvis demonstrated ascites, omental thickening, peritoneal thickening, and mesenteric adenopathy, suggestive of carcinomatosis. She was admitted with a presumed diagnosis of sepsis secondary to pneumonia and started empirically on broad-spectrum antibiotics without clinical improvement. A battery of oncology markers was ordered and revealed a mildly elevated cancer antigen (CA)-125. Diagnostic paracentesis showed lymphocytic predominance with positive mycobacteria PCR, elevated adenosine deaminase (ADA), and no malignant cells. Subsequently, the sputum acid-fast bacilli (AFB) stain returned positive for tuberculosis, confirming the diagnosis of pulmonary tuberculosis. A peritoneal biopsy was obtained and demonstrated caseating granulomas consistent with peritoneal tuberculosis. The patient was started on standard antituberculosis therapy with clinical improvement.</p><p><strong>Conclusions: </strong>This case highlights the need for a high-level of suspicion for peritoneal tuberculosis in a patient with pulmonary tuberculosis who presents with intra-abdominal ascites, omental thickening, peritoneal thickening, and mesenteric lymphadenopathy, despite the presence of an elevated CA-125 level.</p>","PeriodicalId":9608,"journal":{"name":"Case Reports in Infectious Diseases","volume":" ","pages":"7012943"},"PeriodicalIF":0.8000,"publicationDate":"2022-10-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9629952/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Infectious Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/7012943","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
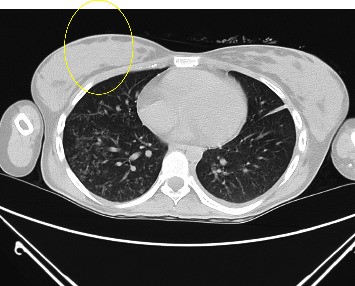
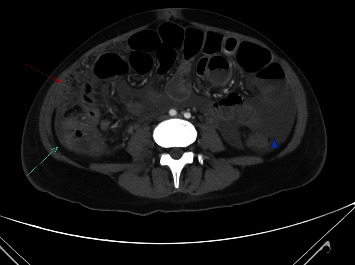
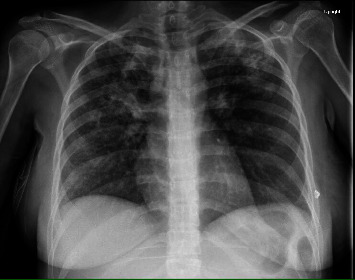
Background: Peritoneal tuberculosis is a rare form of extrapulmonary tuberculosis and presents a challenging diagnosis because of its nonspecific clinical manifestations. Peritoneal TB mimics other pathologies, including abdominal carcinomatosis, especially when the patient presents with ascites and an elevated cancer antigen (CA)-125 levels. Case Presentation. A postpartum 20-year-old Hispanic female recently discharged after transverse cesarean surgery, presented to the ER with fever, chills, edema, abdominal distension, nausea, and vomiting. The patient was febrile, tachycardic, and hypotensive. Chest X-ray demonstrated alveolar and interstitial consolidations; chest CT revealed tree-in-bud opacities in the right lower lobe, suggestive of atypical (TB)/fungal infection. CT of the abdomen and pelvis demonstrated ascites, omental thickening, peritoneal thickening, and mesenteric adenopathy, suggestive of carcinomatosis. She was admitted with a presumed diagnosis of sepsis secondary to pneumonia and started empirically on broad-spectrum antibiotics without clinical improvement. A battery of oncology markers was ordered and revealed a mildly elevated cancer antigen (CA)-125. Diagnostic paracentesis showed lymphocytic predominance with positive mycobacteria PCR, elevated adenosine deaminase (ADA), and no malignant cells. Subsequently, the sputum acid-fast bacilli (AFB) stain returned positive for tuberculosis, confirming the diagnosis of pulmonary tuberculosis. A peritoneal biopsy was obtained and demonstrated caseating granulomas consistent with peritoneal tuberculosis. The patient was started on standard antituberculosis therapy with clinical improvement.
Conclusions: This case highlights the need for a high-level of suspicion for peritoneal tuberculosis in a patient with pulmonary tuberculosis who presents with intra-abdominal ascites, omental thickening, peritoneal thickening, and mesenteric lymphadenopathy, despite the presence of an elevated CA-125 level.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
