Lindsay B. Young , Marcin Kolber , Michael J. King , Mona Ranade , Vivian L. Bishay , Rahul S. Patel , Francis S. Nowakowski , Aaron M. Fischman , Robert A. Lookstein , Edward Kim
{"title":"Intrahepatic flow diversion prior to segmental Yttrium-90 radioembolization for challenging tumor vasculature","authors":"Lindsay B. Young , Marcin Kolber , Michael J. King , Mona Ranade , Vivian L. Bishay , Rahul S. Patel , Francis S. Nowakowski , Aaron M. Fischman , Robert A. Lookstein , Edward Kim","doi":"10.1016/j.jimed.2022.02.001","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Hepatic tumors with complex vascular supply or poor relative perfusion are prone to decreased rates of objective response. This is compounded in the setting of Yttrium-90 (Y90) transarterial radioembolization (TARE), which is minimally embolic and flow-dependent, relying on high threshold dose for complete response.</p></div><div><h3>Objective</h3><p>We describe our experience with intrahepatic flow diversion (FD) prior to TARE of hepatocellular carcinoma (HCC) with challenging vascular supply.</p></div><div><h3>Materials and methods</h3><p>Between April 2014 and January 2020, 886 cases of coinciding MAA or TARE and bland embolization or temporary occlusion were identified. Intraprocedural embolizations performed for more routine purposes were excluded. FD was performed by bland embolization or temporary occlusion of vessels supplying non-malignant parenchyma in cases where flow was not preferential to target tumor. Lesion characteristics, vascular supply, treatment approach, angiography, and adverse events (AEs) were reviewed. Radiographic response was assessed using mRECIST criteria.</p></div><div><h3>Results</h3><p>22 cases of FD of focal HCC were identified. Embolics included calibrated microspheres (n = 11), microcoils (n = 4), gelfoam (n = 3), temporary balloon occlusion (n = 2) and temporary deployment of a microvascular plug (n = 1). Post-treatment SPECT-CT dosimetry coverage was concordant with target lesions in all cases. Mean follow-up was 16.7 months (1.4–45 mos). Tumor-specific response per mRECIST was 41% complete response, 50% objective response, and 59% disease control rate. No major adverse events or grade 3/4 hepatotoxicity were reported.</p></div><div><h3>Conclusion</h3><p>Our findings suggest that FD prior to TARE is safe and potentially effective in treating HCC with complex vascular supply or poor tumor perfusion.</p></div>","PeriodicalId":33533,"journal":{"name":"Journal of Interventional Medicine","volume":"5 2","pages":"Pages 79-83"},"PeriodicalIF":0.0000,"publicationDate":"2022-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9349007/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Medicine","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2096360222000096","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
Background
Hepatic tumors with complex vascular supply or poor relative perfusion are prone to decreased rates of objective response. This is compounded in the setting of Yttrium-90 (Y90) transarterial radioembolization (TARE), which is minimally embolic and flow-dependent, relying on high threshold dose for complete response.
Objective
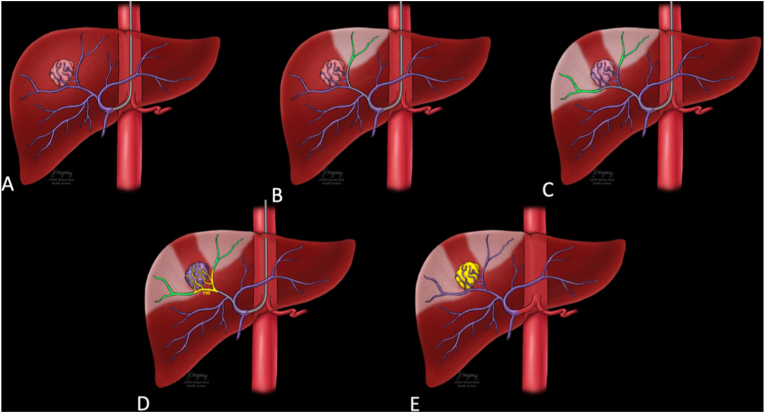
We describe our experience with intrahepatic flow diversion (FD) prior to TARE of hepatocellular carcinoma (HCC) with challenging vascular supply.
Materials and methods
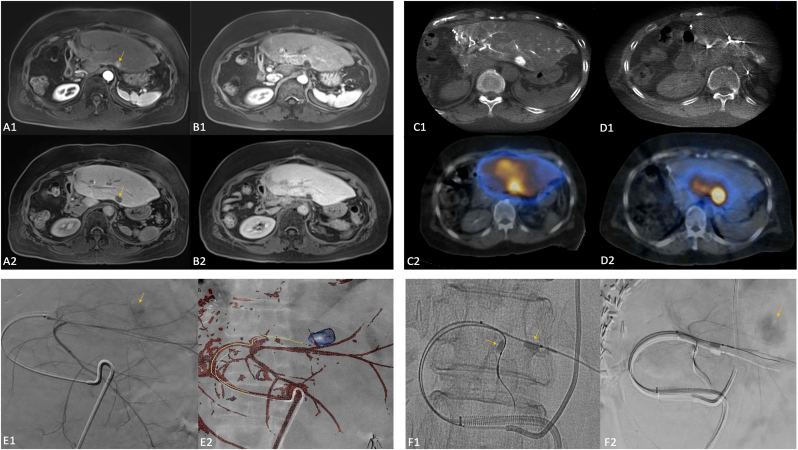
Between April 2014 and January 2020, 886 cases of coinciding MAA or TARE and bland embolization or temporary occlusion were identified. Intraprocedural embolizations performed for more routine purposes were excluded. FD was performed by bland embolization or temporary occlusion of vessels supplying non-malignant parenchyma in cases where flow was not preferential to target tumor. Lesion characteristics, vascular supply, treatment approach, angiography, and adverse events (AEs) were reviewed. Radiographic response was assessed using mRECIST criteria.
Results
22 cases of FD of focal HCC were identified. Embolics included calibrated microspheres (n = 11), microcoils (n = 4), gelfoam (n = 3), temporary balloon occlusion (n = 2) and temporary deployment of a microvascular plug (n = 1). Post-treatment SPECT-CT dosimetry coverage was concordant with target lesions in all cases. Mean follow-up was 16.7 months (1.4–45 mos). Tumor-specific response per mRECIST was 41% complete response, 50% objective response, and 59% disease control rate. No major adverse events or grade 3/4 hepatotoxicity were reported.
Conclusion
Our findings suggest that FD prior to TARE is safe and potentially effective in treating HCC with complex vascular supply or poor tumor perfusion.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
