Telemonitoring of Elderly with Hypertension and Type 2 Diabetes at the Primary Care Level: Protocol for a Multicentric Randomized Controlled Pilot Study.
Matic Mihevc, Črt Zavrnik, Majda Mori Lukančič, Tina Virtič, Valentina Prevolnik Rupel, Marija Petek Šter, Zalika Klemenc Ketiš, Antonija Poplas Susič
{"title":"Telemonitoring of Elderly with Hypertension and Type 2 Diabetes at the Primary Care Level: Protocol for a Multicentric Randomized Controlled Pilot Study.","authors":"Matic Mihevc, Črt Zavrnik, Majda Mori Lukančič, Tina Virtič, Valentina Prevolnik Rupel, Marija Petek Šter, Zalika Klemenc Ketiš, Antonija Poplas Susič","doi":"10.2478/sjph-2022-0029","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Arterial hypertension (AH) and type 2 diabetes (T2D) represent a significant burden for the public health system, with an exceptionally high prevalence in patients aged ≥65 years. This study aims to test the acceptability, clinical effectiveness, and cost-effectiveness of telemonitoring in elderly patients with AH and T2D at the primary care level.</p><p><strong>Methods: </strong>A m ulti-centre, prospective, randomized, controlled t rial w ill be conducted. Patients a ged ≥ 65 y ears with AH and T2D will be randomized in a 1:1 proportion to a mHealth intervention or standard care group. Patients in the intervention group will measure their blood pressure (BP) twice weekly and blood glucose (BG) once monthly. The readings will be synchronously transmitted via a mobile application to the telemonitoring platform, where they will be reviewed by a general practitioner who will indicate changes in measurement regimen or carry out a teleconsultation. The primary endpoint will be a change in systolic BP (SBP) and glycated haemoglobin (HbA1c) relative to standard care up to 12 months after inclusion. Secondary endpoints will be a change in other observed clinical variables, quality-of-life indexes, and costs.</p><p><strong>Expected results: </strong>Telemonitoring will be an acceptable method of care associated with significant reductions in SBP and HbA1c levels and an increase in quality-of-life indexes in the intervention group. However, the cost-effectiveness threshold (incremental cost-effectiveness ratio below €25,000/quality-adjusted life year) might not be reached.</p><p><strong>Conclusion: </strong>This study will provide new evidence for scaling up telemonitoring network at the primary care level and modifying telemonitoring protocols to achieve the best clinical and cost-effective outcomes.</p>","PeriodicalId":45127,"journal":{"name":"Zdravstveno Varstvo","volume":"61 4","pages":"216-223"},"PeriodicalIF":2.4000,"publicationDate":"2022-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f0/41/sjph-61-216.PMC9597900.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Zdravstveno Varstvo","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2478/sjph-2022-0029","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/12/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 2
Abstract
Introduction: Arterial hypertension (AH) and type 2 diabetes (T2D) represent a significant burden for the public health system, with an exceptionally high prevalence in patients aged ≥65 years. This study aims to test the acceptability, clinical effectiveness, and cost-effectiveness of telemonitoring in elderly patients with AH and T2D at the primary care level.
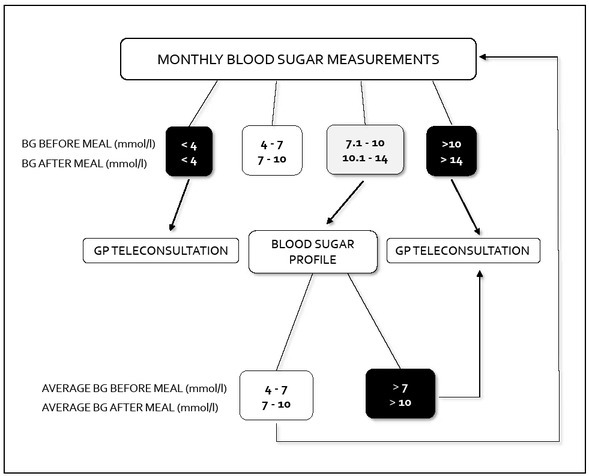
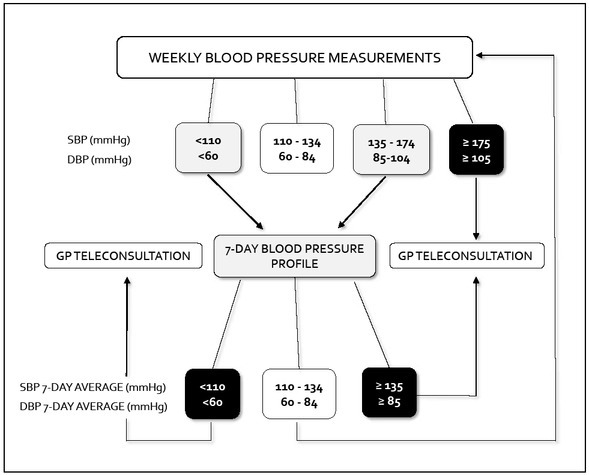
Methods: A m ulti-centre, prospective, randomized, controlled t rial w ill be conducted. Patients a ged ≥ 65 y ears with AH and T2D will be randomized in a 1:1 proportion to a mHealth intervention or standard care group. Patients in the intervention group will measure their blood pressure (BP) twice weekly and blood glucose (BG) once monthly. The readings will be synchronously transmitted via a mobile application to the telemonitoring platform, where they will be reviewed by a general practitioner who will indicate changes in measurement regimen or carry out a teleconsultation. The primary endpoint will be a change in systolic BP (SBP) and glycated haemoglobin (HbA1c) relative to standard care up to 12 months after inclusion. Secondary endpoints will be a change in other observed clinical variables, quality-of-life indexes, and costs.
Expected results: Telemonitoring will be an acceptable method of care associated with significant reductions in SBP and HbA1c levels and an increase in quality-of-life indexes in the intervention group. However, the cost-effectiveness threshold (incremental cost-effectiveness ratio below €25,000/quality-adjusted life year) might not be reached.
Conclusion: This study will provide new evidence for scaling up telemonitoring network at the primary care level and modifying telemonitoring protocols to achieve the best clinical and cost-effective outcomes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
