Rupa Mehta, Karthik Nagaraga Rao, Nitin M Nagarkar, Anil Sharma, Badal Kumar, P Karthik
{"title":"Outcomes of Open Fronto-Facial Resection for Fungal Osteomyelitis of Frontal Bone.","authors":"Rupa Mehta, Karthik Nagaraga Rao, Nitin M Nagarkar, Anil Sharma, Badal Kumar, P Karthik","doi":"10.5041/RMMJ.10484","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The second wave of coronavirus disease 2019 (COVID-19) led to the resurgence of opportunistic infections due to the injudicious use of steroids. Sinonasal mucormycosis was declared an epidemic in India during the pandemic. Mucormycosis was managed effectively by surgical debridement along with systemic amphotericin B. Currently, a resurgence of mucormycosis following initial treatment, in the form of fungal osteomyelitis of the frontal bone, is being seen in India.</p><p><strong>Methods: </strong>This prospective study included 10 patients with fungal osteomyelitis of the frontal bone due to mucormycosis. All patients underwent surgical debridement of the sequestrum and involucrum, with systemic antifungal pharmacotherapy.</p><p><strong>Results: </strong>The average duration of time until mucormycosis recurrence was 22 days following initial treatment (range 10-33 days). Patients presented with extracranial bossing following outer frontal cortex erosion (n=3), bicortical erosion (n=3), bifrontal involvement (n=2), dural involvement (n=3), and involvement of the brain parenchyma and prefrontal cortex (n=2). All cases underwent debridement of the entire sequestrous bone and involucrum until normal bone could be identified. The mean admission duration was 4 weeks (range 3-6 weeks). All treated patients are currently alive and without disease, confirmed by contrast-enhanced computed tomography.</p><p><strong>Conclusion: </strong>Based on our experience, the successful treatment of fungal osteomyelitis due to mucormycosis requires a four-pronged approach: early detection, multidisciplinary management of comorbidities, surgical debridement of necrotic bone, and adequate systemic antifungal therapy.</p>","PeriodicalId":46408,"journal":{"name":"Rambam Maimonides Medical Journal","volume":"13 4","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2022-10-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9622391/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Rambam Maimonides Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5041/RMMJ.10484","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The second wave of coronavirus disease 2019 (COVID-19) led to the resurgence of opportunistic infections due to the injudicious use of steroids. Sinonasal mucormycosis was declared an epidemic in India during the pandemic. Mucormycosis was managed effectively by surgical debridement along with systemic amphotericin B. Currently, a resurgence of mucormycosis following initial treatment, in the form of fungal osteomyelitis of the frontal bone, is being seen in India.
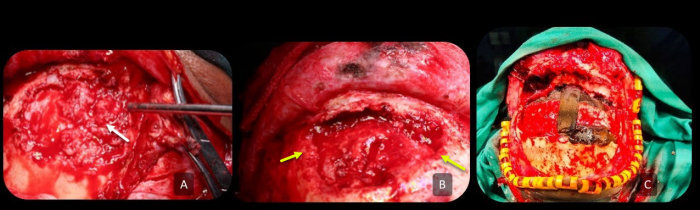
Methods: This prospective study included 10 patients with fungal osteomyelitis of the frontal bone due to mucormycosis. All patients underwent surgical debridement of the sequestrum and involucrum, with systemic antifungal pharmacotherapy.
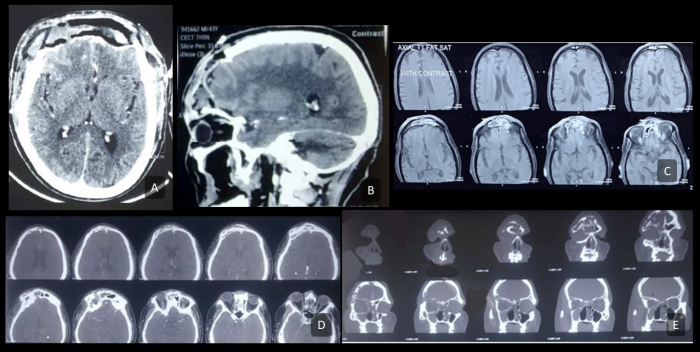
Results: The average duration of time until mucormycosis recurrence was 22 days following initial treatment (range 10-33 days). Patients presented with extracranial bossing following outer frontal cortex erosion (n=3), bicortical erosion (n=3), bifrontal involvement (n=2), dural involvement (n=3), and involvement of the brain parenchyma and prefrontal cortex (n=2). All cases underwent debridement of the entire sequestrous bone and involucrum until normal bone could be identified. The mean admission duration was 4 weeks (range 3-6 weeks). All treated patients are currently alive and without disease, confirmed by contrast-enhanced computed tomography.
Conclusion: Based on our experience, the successful treatment of fungal osteomyelitis due to mucormycosis requires a four-pronged approach: early detection, multidisciplinary management of comorbidities, surgical debridement of necrotic bone, and adequate systemic antifungal therapy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
