Marco Alejandro Jimenez-Ochoa, Maria Margarita Contreras-Serratos, Martha Leticia Gonzalez-Bautista, Constantino Lopez-Macias, Diego Alberto Lozano-Jaramillo
{"title":"Isolated Renal Relapse in a Post-Allogenic Transplant Adult Patient With Acute Lymphoblastic Leukemia.","authors":"Marco Alejandro Jimenez-Ochoa, Maria Margarita Contreras-Serratos, Martha Leticia Gonzalez-Bautista, Constantino Lopez-Macias, Diego Alberto Lozano-Jaramillo","doi":"10.14740/jmc4003","DOIUrl":null,"url":null,"abstract":"<p><p>Acute lymphoblastic leukemia (ALL) is an aggressive hematological neoplasm typically more common in children than adults. More prolonged remissions and a potential cure can be achieved if allogeneic hematopoietic stem cell transplantation (allo-HSCT) is performed. Outcomes after allo-HSCT vary significantly among patients, and multiple factors contribute to these outcomes. Isolated extramedullary relapse (iEMR) after allo-HSCT is rare. We present the case of a 43-year-old man who was diagnosed with Philadelphia chromosome-negative (Ph-neg), B-cell ALL and underwent haploidentical allo-HSCT because of high-risk features at diagnosis. One year later, he was admitted to the hospital with facial and peripheral edema, proteinuria, elevated serum creatinine levels, and hypertension. Renal biopsy was performed immediately. Renal infiltration of TdT+ leukemic cells was detected by immunohistochemistry. Bone marrow aspiration, lumbar puncture, and computed tomography (CT) scans were performed to identify other sites of possible relapse. No other sites were identified, and an extramedullary isolated renal relapse was diagnosed. Intensive re-induction with chemotherapy was not possible because of the coronavirus disease 2019 (COVID-19) infection. Six weeks later, a medullary relapse was noted. Medullary infiltration of B-cell ALL after allo-HSCT has a historically poor prognosis; however, iEMR appears to have a better overall prognosis. The optimal treatment for renal iEMR is still a matter of debate.</p>","PeriodicalId":16279,"journal":{"name":"Journal of Medical Cases","volume":"13 10","pages":"499-503"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5b/70/jmc-13-499.PMC9635765.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4003","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
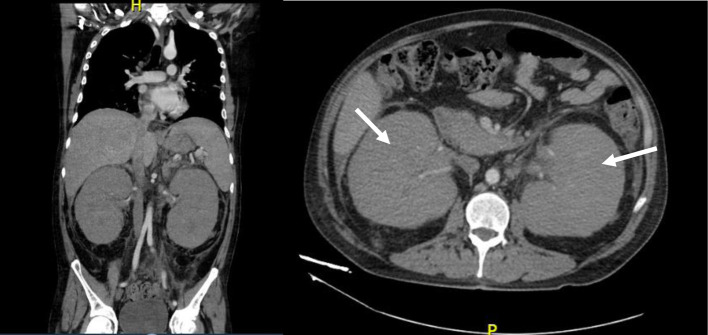
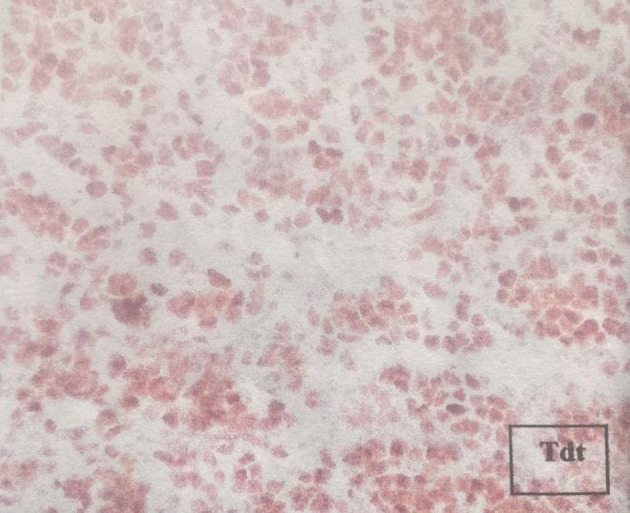
Acute lymphoblastic leukemia (ALL) is an aggressive hematological neoplasm typically more common in children than adults. More prolonged remissions and a potential cure can be achieved if allogeneic hematopoietic stem cell transplantation (allo-HSCT) is performed. Outcomes after allo-HSCT vary significantly among patients, and multiple factors contribute to these outcomes. Isolated extramedullary relapse (iEMR) after allo-HSCT is rare. We present the case of a 43-year-old man who was diagnosed with Philadelphia chromosome-negative (Ph-neg), B-cell ALL and underwent haploidentical allo-HSCT because of high-risk features at diagnosis. One year later, he was admitted to the hospital with facial and peripheral edema, proteinuria, elevated serum creatinine levels, and hypertension. Renal biopsy was performed immediately. Renal infiltration of TdT+ leukemic cells was detected by immunohistochemistry. Bone marrow aspiration, lumbar puncture, and computed tomography (CT) scans were performed to identify other sites of possible relapse. No other sites were identified, and an extramedullary isolated renal relapse was diagnosed. Intensive re-induction with chemotherapy was not possible because of the coronavirus disease 2019 (COVID-19) infection. Six weeks later, a medullary relapse was noted. Medullary infiltration of B-cell ALL after allo-HSCT has a historically poor prognosis; however, iEMR appears to have a better overall prognosis. The optimal treatment for renal iEMR is still a matter of debate.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
