{"title":"Super-refractory status epilepticus in adults.","authors":"Michael P Malter, Janina Neuneier","doi":"10.1186/s42466-022-00199-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Super-refractory status epilepticus (SRSE) represents the culmination of refractory status epilepticus (RSE) and carries a significant risk of poor neurological outcome and high mortality. RSE is not defined primarily by seizure duration, but by failure to respond to appropriate antiseizure treatment. SRSE is present when a RSE persists or recurs after more than 24 h of treatment with anesthetics. No evidence-based treatment algorithms can be provided for SRSE. Therefore, we propose a pragmatic standard operating procedure (SOP) for the management of SRSE that addresses the existing uncertainties in the treatment of SRSE and provides options for resolution and decision-making.</p><p><strong>Comments: </strong>First, we recommend the assessment of persistent seizure activity and the evaluation of differential diagnoses to confirm correct diagnosis. Relevant differential diagnoses include psychogenic non-epileptic seizures, hypoxic, metabolic, or toxic encephalopathies, and tetanus. During SE or in severe encephalopathies, a so-called electroclinical ictal-interictal continuum may occur, which denotes an intermediate stage that cannot be defined with certainty as ictal or interictal by EEG and should not lead to harmful overtreatment. Because both prognosis and specific treatment options depend crucially on the etiology of SRSE, the etiological evaluation should be performed rapidly. When SRSE is confirmed, various pharmacological and non-pharmacological treatment options are available.</p><p><strong>Conclusion: </strong>We provide a pragmatical SOP for adult people with SRSE.</p>","PeriodicalId":19169,"journal":{"name":"Neurological Research and Practice","volume":" ","pages":"35"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9394073/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurological Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42466-022-00199-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
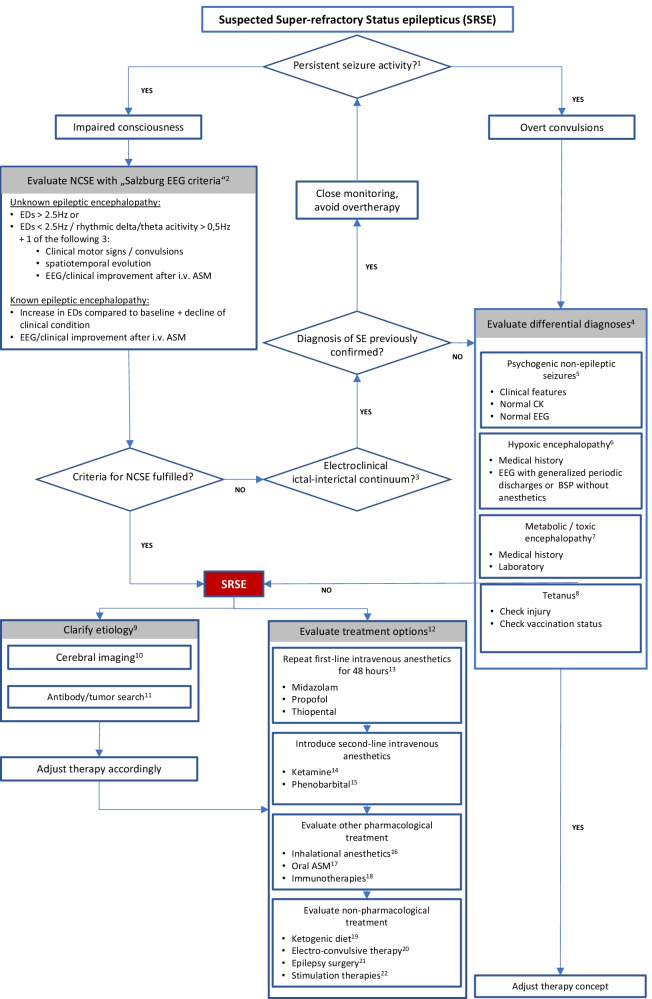
Introduction: Super-refractory status epilepticus (SRSE) represents the culmination of refractory status epilepticus (RSE) and carries a significant risk of poor neurological outcome and high mortality. RSE is not defined primarily by seizure duration, but by failure to respond to appropriate antiseizure treatment. SRSE is present when a RSE persists or recurs after more than 24 h of treatment with anesthetics. No evidence-based treatment algorithms can be provided for SRSE. Therefore, we propose a pragmatic standard operating procedure (SOP) for the management of SRSE that addresses the existing uncertainties in the treatment of SRSE and provides options for resolution and decision-making.
Comments: First, we recommend the assessment of persistent seizure activity and the evaluation of differential diagnoses to confirm correct diagnosis. Relevant differential diagnoses include psychogenic non-epileptic seizures, hypoxic, metabolic, or toxic encephalopathies, and tetanus. During SE or in severe encephalopathies, a so-called electroclinical ictal-interictal continuum may occur, which denotes an intermediate stage that cannot be defined with certainty as ictal or interictal by EEG and should not lead to harmful overtreatment. Because both prognosis and specific treatment options depend crucially on the etiology of SRSE, the etiological evaluation should be performed rapidly. When SRSE is confirmed, various pharmacological and non-pharmacological treatment options are available.
Conclusion: We provide a pragmatical SOP for adult people with SRSE.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
