{"title":"Development of a Predictive Model for Common Bile Duct Stones in Patients With Clinical Suspicion of Choledocholithiasis: A Cohort Study.","authors":"Suppadech Tunruttanakul, Kotchakorn Verasmith, Jayanton Patumanond, Chatchai Mingmalairak","doi":"10.14740/gr1560","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Current choledocholithiasis guidelines heavily focus on patients with low or no risk, they may be inappropriate for populations with high rates of choledocholithiasis. We aimed to develop a predictive scoring model for choledocholithiasis in patients with relevant clinical manifestations.</p><p><strong>Methods: </strong>A multivariable predictive model development study based on a retrospective cohort of patients with clinical suspicion of choledocholithiasis was used in this study. The setting was a 700-bed public tertiary hospital. Participants were patients who had completed three reference tests (endoscopic retrograde cholangiography, magnetic resonance cholangiopancreatography, and intraoperative cholangiography) from January 2019 to June 2021. The model was developed using logistic regression analysis. Predictor selection was conducted using a backward stepwise approach. Three risk groups were considered. Model performance was evaluated by area under the receiver operating characteristic curve, calibration, classification measures, and decision curve analyses.</p><p><strong>Results: </strong>Six hundred twenty-one patients were included; the choledocholithiasis prevalence was 59.9%. The predictors were age > 55 years, pancreatitis, cholangitis, cirrhosis, alkaline phosphatase level of 125 - 250 or > 250 U/L, total bilirubin level > 4 mg/dL, common bile duct size > 6 mm, and common bile duct stone detection. Pancreatitis and cirrhosis each had a negative score. The sum of scores was -4.5 to 28.5. Patients were categorized into three risk groups: low-intermediate (score ≤ 5), intermediate (score 5.5 - 14.5), and high (score ≥ 15). Positive likelihood ratios were 0.16 and 3.47 in the low-intermediate and high-risk groups, respectively. The model had an area under the receiver operating characteristic curve of 0.80 (95% confidence interval: 0.76, 0.83) and was well-calibrated; it exhibited better statistical suitability to the high-prevalence population, compared to current guidelines.</p><p><strong>Conclusions: </strong>Our scoring model had good predictive ability for choledocholithiasis in patients with relevant clinical manifestations. Consideration of other factors is necessary for clinical application, particularly regarding the availability of expert physicians and specialized equipment.</p>","PeriodicalId":12461,"journal":{"name":"Gastroenterology Research","volume":"15 5","pages":"240-252"},"PeriodicalIF":1.7000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/be/78/gr-15-240.PMC9635785.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/gr1560","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/19 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Current choledocholithiasis guidelines heavily focus on patients with low or no risk, they may be inappropriate for populations with high rates of choledocholithiasis. We aimed to develop a predictive scoring model for choledocholithiasis in patients with relevant clinical manifestations.
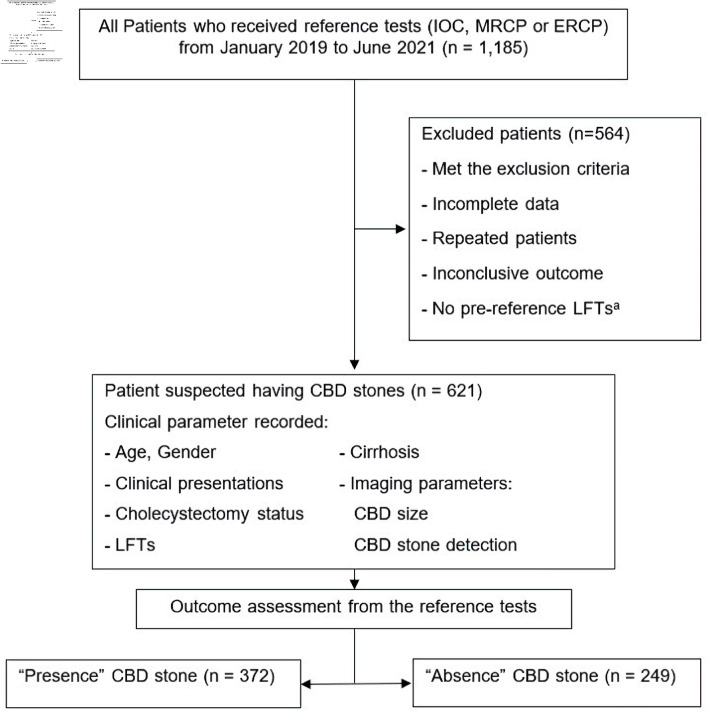
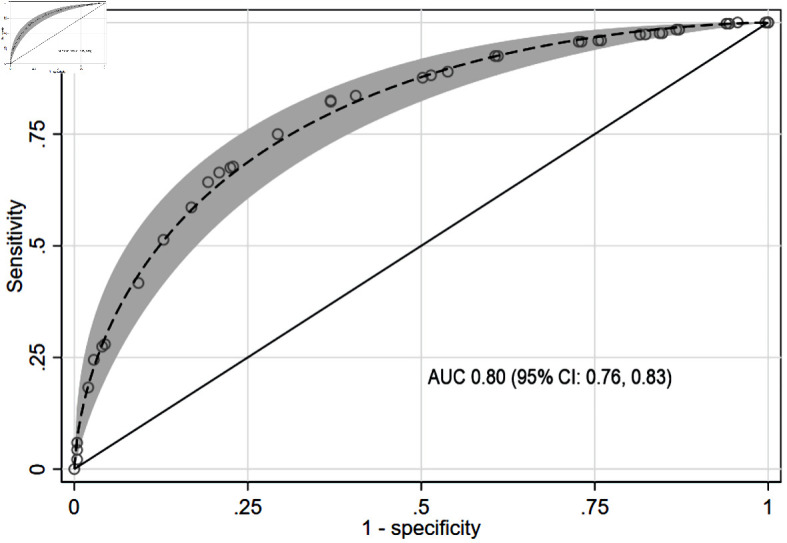
Methods: A multivariable predictive model development study based on a retrospective cohort of patients with clinical suspicion of choledocholithiasis was used in this study. The setting was a 700-bed public tertiary hospital. Participants were patients who had completed three reference tests (endoscopic retrograde cholangiography, magnetic resonance cholangiopancreatography, and intraoperative cholangiography) from January 2019 to June 2021. The model was developed using logistic regression analysis. Predictor selection was conducted using a backward stepwise approach. Three risk groups were considered. Model performance was evaluated by area under the receiver operating characteristic curve, calibration, classification measures, and decision curve analyses.
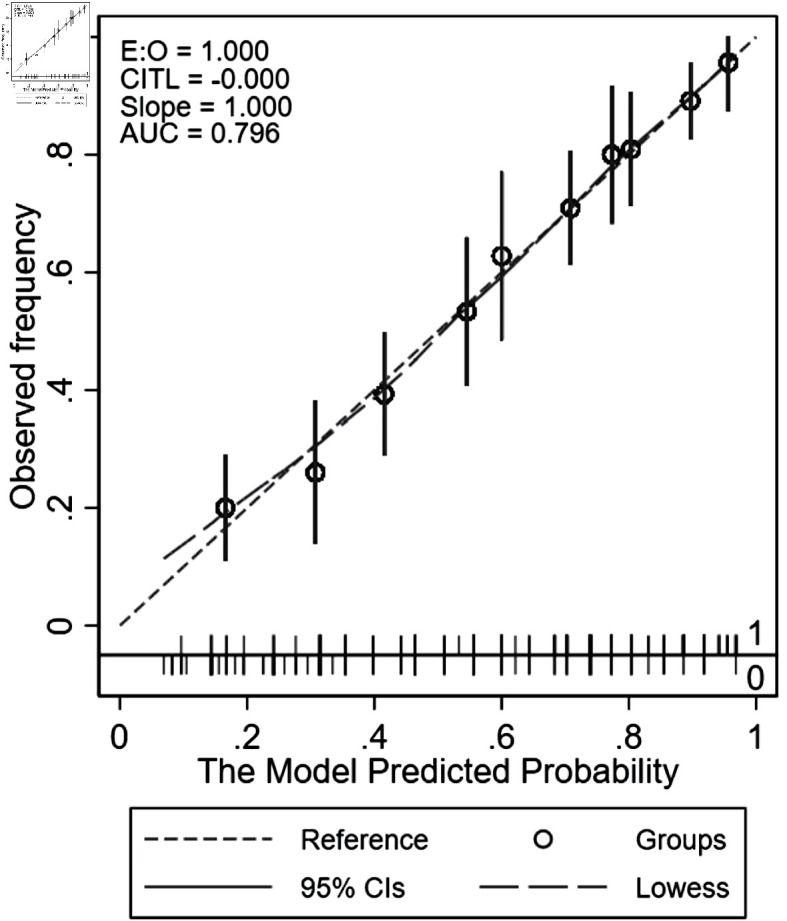
Results: Six hundred twenty-one patients were included; the choledocholithiasis prevalence was 59.9%. The predictors were age > 55 years, pancreatitis, cholangitis, cirrhosis, alkaline phosphatase level of 125 - 250 or > 250 U/L, total bilirubin level > 4 mg/dL, common bile duct size > 6 mm, and common bile duct stone detection. Pancreatitis and cirrhosis each had a negative score. The sum of scores was -4.5 to 28.5. Patients were categorized into three risk groups: low-intermediate (score ≤ 5), intermediate (score 5.5 - 14.5), and high (score ≥ 15). Positive likelihood ratios were 0.16 and 3.47 in the low-intermediate and high-risk groups, respectively. The model had an area under the receiver operating characteristic curve of 0.80 (95% confidence interval: 0.76, 0.83) and was well-calibrated; it exhibited better statistical suitability to the high-prevalence population, compared to current guidelines.
Conclusions: Our scoring model had good predictive ability for choledocholithiasis in patients with relevant clinical manifestations. Consideration of other factors is necessary for clinical application, particularly regarding the availability of expert physicians and specialized equipment.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
