{"title":"Serine supplementation: Is it a new option for the treatment of diabetic polyneuropathy?","authors":"Hiroki Mizukami","doi":"10.1111/jdi.14047","DOIUrl":null,"url":null,"abstract":"<p>Subjects with diabetes develop marked disturbances in amino acid metabolism and the concentration in plasma and tissues. Most consistently, the levels of branched-chain amino acids (BCAAs) and aromatic amino acids are increased, and the levels of <span>l</span>-serine and glycine are decreased<span><sup>1</sup></span>. Aberrant nonessential amino acid metabolism is involved in the pathogenesis of diabetes. Elevated levels of plasma BCAAs have been associated with insulin resistance and type 2 diabetes since the 1960s<span><sup>2</sup></span>. A cluster of obesity-associated changes in the specific amino acid, acylcarnitine, and organic acid metabolites in obese compared with lean subjects was also associated with insulin resistance. Although it is also speculated that disturbances in aminoacidemia play a role in the development of diabetic complications, their pathogenesis has not been sufficiently elucidated in detail.</p><p>Diabetic peripheral neuropathy (DPN) is the most frequent complication among diabetic patients. Its symptoms are pain, hyperalgesia, hypoalgesia, and paralysis, which can decrease the quality of life of patients. In diabetic peripheral neuropathy, peripheral nerve fibers are affected from the prediabetic stage. Because diabetic peripheral neuropathy is a retrograde-type neuropathy, small nerve fibers located in the epidermis or cornea are first degraded. Small nerve fibers consist of myelinated Aδ fibers and unmyelinated C fibers. Small fiber neuropathy is a disorder of these nerve fibers, manifesting as spontaneous pain or loss of pain sensation with reduction of their density. As diabetic peripheral neuropathy progresses, large myelinated fibers are also decreased with segmental demyelination and microvascular changes, such as thickening of the vascular wall and stenosis of intraneuronal vessels. Without proper treatment, these patients develop paralysis or ulcer formation on the foot. To date, diabetic peripheral neuropathy is thought to be caused by aberrant glucose metabolism in neuronal cells, Schwann cells and endothelial cells in the peripheral nervous system. Abnormal glycemic metabolism elicits nerve dysfunction with activation of the polyol pathway, protein kinase C, advanced glycation end products and its receptor, the receptor for advanced glycation end product (RAGE) pathway, oxidative stress, and inflammation. Clinically, in addition to hyperglycemia, metabolic syndrome, including dyslipidemia, obesity and hypertension, is well known to be a contributor to the pathogenesis of diabetic peripheral neuropathy. In addition to glucose and fatty acid metabolism, recent metabolomics studies have revealed the involvement of another metabolite, glucosamine, in the pathogenesis of diabetic peripheral neuropathy. Lower baseline amino acid levels such as asparagine and glutamine were correlated with cardiovascular autonomic neuropathy in a small sample of subjects with type 1 diabetes<span><sup>3</sup></span>. Thus, today, it is recognized that the pathogenesis of diabetic peripheral neuropathy is not caused only by abnormal glucose metabolism but is a complex condition in which metabolic failure of other nutrients is involved. However, the full picture of the specific metabolic changes in diabetic peripheral neuropathy has not yet been elucidated.</p><p>In this context, Handzlik <i>et al</i>.<span><sup>4</sup></span> recently reported in <i>Nature</i> that the combination of serine deficiency and dyslipidemia can cause experimental diabetic peripheral neuropathy mainly consisting of small fiber neuropathy, in which serine supplementation can delay the onset (Figure 1). The <i>db/db</i> mouse model, which is a conventional obese type 2 diabetic model, showed reductions in hepatic and renal serine levels by approximately 30% relative to wild-type mice, and glycine pools were reduced by 30–50% in the liver, kidney, inguinal white adipose tissue, and plasma. The expression level of components encoding the glycine cleavage system was increased in <i>db/db</i> liver, whereas the expression of genes associated with <i>de novo</i> serine synthesis was significantly reduced. These results indicate that serine synthesis is limited in diabetic mice. Although streptozotocin (STZ)-induced type 1 diabetic model mice showed alterations in plasma glycine and BCAAs (but not serine) at 1 week after streptozotocin treatment, elevated serine disposal was confirmed by co-administration of glucose and serine 2 weeks after injection. Thus, insulin resistance or deficiency can both contribute to the acceleration of serine catabolism or the disposal and reduction of circulating serine in diabetic mice. Of note, weight gain caused by a high-fat diet (HFD) was attenuated by dietary serine and glycine restriction with a reduction in fat mass but not lean mass relative to the treatment with HFD alone, whereas food, calorie, and water intake; calorie absorption; insulin and glucose tolerance; and physical activity were all unaffected. Recent reports suggest that changes in the microbiome composition in the gut can be involved in the pathogenesis of small fiber neuropathy or diabetic peripheral neuropathy<span><sup>5</sup></span>. Investigation of the fecal microbiome revealed that the log ratios of the strains of microorganisms expressing complete serine biosynthesis were increased, while glycine cleavage pathways were decreased with a reduction in the strains expressing a complete fatty acid synthesis pathway by treatment with a serine- and glycine-restricted HFD.</p><p>Serine catabolism is associated with sphingolipid metabolism <i>via</i> serine palmitoyl transferase. Sphingolipids are abundantly contained in the myelin sheath in peripheral nerves. Restriction of dietary serine and glycine reduced hepatic palmitate synthesis by approximately 70% relative to serine-replete control diets. Hepatic cholesterol synthesis was increased in the serine-free HFD group compared with the HFD group, with a reduction in the expression of cholesterol biosynthesis enzymes and an increase or no change in the expression of cholesterol biosynthesis enzymes.</p><p>Recently, the involvement of insulin resistance in the peripheral nerves has been reported in diabetic peripheral neuropathy, in which proinflammatory macrophage infiltration activated by RAGE signaling elicits deficits in retrograde axonal transportation. Because serine and glycine levels were less associated with changes in protein kinase B phosphorylation than dietary fat and carbohydrate contents, serine restriction could evoke changes in fatty acid metabolism independent of insulin signaling.</p><p>Serine deficiency is known to be associated with peripheral neuropathy and various neurodegenerative disorders in previous clinical studies. Similarly, mice fed serine- and glycine-free low-fat chow diets for 12 months exhibited thermal hypoalgesia with intraepidermal nerve fiber reduction in the paw skin. Interestingly, a HFD accelerated the thermal hypoalgesia in mice fed a serine- and glycine-restricted diet for just 3 months. These findings indicate that a combination of low systemic serine and HFD feeding accelerates the onset of small fiber neuropathy in mice. The authors further explored the metabolic changes associated with neuropathy caused by serine restriction. 1-Deoxysphingolipids, including deoxydihydroceramides, are neurotoxic sphingolipids. A 1-deoxysphingolipid is produced when the first enzyme of the sphingolipid biosynthetic pathway, serine palmitoyltransferase, uses <span>l</span>-alanine as a substrate instead of its canonical amino acid substrate, serine. As expected, the contents of deoxydihydro-ceramides in the liver and paw skin increased in serine- and glycine-restricted mice fed HFD, while the canonical ceramide content was reduced. Administration of an inhibitor of serine palmitoyl transferase (myriocin) strongly reduced the levels of sphingolipids as well as of triglycerides and diacylglycerides. Myriocin ameliorated thermal hypoalgesia and the small fiber nerve density in serine- and glycine-restricted HFD mice, while myriocin had no impact on tactile sensing or nerve conduction velocities. Importantly, the administration of myriocin at 6 weeks of age prevented the manifestation of thermal hypoalgesia, tactile sensation, and small fiber density in the epidermis in <i>db/db</i> mice without affecting body weight gain, hyperglycemia, or plasma serine levels. Myriosin treatment strongly reduced canonical sphingolipids in the liver but showed limited effects on paw skin 1-deoxysphingolipids and ceramides. Finally, based on the results obtained thus far, the authors investigated whether a serine-supplemented diet prevents the development of neuropathy. A 3% serine-enriched diet starting at 6 weeks of age elevated levels of plasma and hepatic serine, but not glycine levels. The body weight was comparable, while a slight increase in circulating glucose levels was observed. Neuropathic manifestations, including both thermal and tactile hypoalgesia, were reduced in diabetic mice fed this serine-enriched diet. Canonical sphingolipid levels were similar across the tissues, while 1-deoxysphingolipids were robustly decreased in both liver and paw skin. Collectively, these data suggest that supplementation with serine can prevent the onset and progression of diabetic peripheral neuropathy.</p><p>The novel point of this research is that the onset of diabetic peripheral neuropathy could be prevented by correcting the intake of nutrients without affecting blood glucose levels. Currently, no radical therapy for diabetic peripheral neuropathy has been established. Although aldose reductase inhibitors and α-lipoic acid have been clinically applied, their effects are limited. This study suggests that the decrease in serine synthesis and the increase in serine disposal are due to insufficient action of insulin. Although the most important treatment for neuropathy is glycemic control of diabetes itself, it may be necessary to consider treatment of diabetic peripheral neuropathy with a focus on improving insulin action in more organs.</p><p>The results of this study also indicate that nutrient factors other than glucose and lipids will accelerate the onset and development of diabetic peripheral neuropathy. This explains one of the reasons why the progression of neuropathy cannot be suppressed by glycemic control alone. Conversely, serine supplementation can prevent the onset of neuropathy to some extent, but not completely in this report. These results reconfirm that diabetic peripheral neuropathy is a multifactorial disease. Therefore, it is conceivable that serine could be administered as an adjunctive therapy in addition to glycemic control.</p><p>Unfortunately, the results of this study only relate to the prevention of the onset and progression of experimental diabetic peripheral neuropathy by serine supplementation or myriocin administration, and they do not constitute a treatment. In the future, it will be necessary to evaluate whether correcting serine metabolism can alleviate diabetic peripheral neuropathy that has already developed and progressed or to confirm the efficacy in prospective clinical research.</p>","PeriodicalId":190,"journal":{"name":"Journal of Diabetes Investigation","volume":"14 10","pages":"1157-1159"},"PeriodicalIF":3.0000,"publicationDate":"2023-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jdi.14047","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Diabetes Investigation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jdi.14047","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Subjects with diabetes develop marked disturbances in amino acid metabolism and the concentration in plasma and tissues. Most consistently, the levels of branched-chain amino acids (BCAAs) and aromatic amino acids are increased, and the levels of l-serine and glycine are decreased1. Aberrant nonessential amino acid metabolism is involved in the pathogenesis of diabetes. Elevated levels of plasma BCAAs have been associated with insulin resistance and type 2 diabetes since the 1960s2. A cluster of obesity-associated changes in the specific amino acid, acylcarnitine, and organic acid metabolites in obese compared with lean subjects was also associated with insulin resistance. Although it is also speculated that disturbances in aminoacidemia play a role in the development of diabetic complications, their pathogenesis has not been sufficiently elucidated in detail.
Diabetic peripheral neuropathy (DPN) is the most frequent complication among diabetic patients. Its symptoms are pain, hyperalgesia, hypoalgesia, and paralysis, which can decrease the quality of life of patients. In diabetic peripheral neuropathy, peripheral nerve fibers are affected from the prediabetic stage. Because diabetic peripheral neuropathy is a retrograde-type neuropathy, small nerve fibers located in the epidermis or cornea are first degraded. Small nerve fibers consist of myelinated Aδ fibers and unmyelinated C fibers. Small fiber neuropathy is a disorder of these nerve fibers, manifesting as spontaneous pain or loss of pain sensation with reduction of their density. As diabetic peripheral neuropathy progresses, large myelinated fibers are also decreased with segmental demyelination and microvascular changes, such as thickening of the vascular wall and stenosis of intraneuronal vessels. Without proper treatment, these patients develop paralysis or ulcer formation on the foot. To date, diabetic peripheral neuropathy is thought to be caused by aberrant glucose metabolism in neuronal cells, Schwann cells and endothelial cells in the peripheral nervous system. Abnormal glycemic metabolism elicits nerve dysfunction with activation of the polyol pathway, protein kinase C, advanced glycation end products and its receptor, the receptor for advanced glycation end product (RAGE) pathway, oxidative stress, and inflammation. Clinically, in addition to hyperglycemia, metabolic syndrome, including dyslipidemia, obesity and hypertension, is well known to be a contributor to the pathogenesis of diabetic peripheral neuropathy. In addition to glucose and fatty acid metabolism, recent metabolomics studies have revealed the involvement of another metabolite, glucosamine, in the pathogenesis of diabetic peripheral neuropathy. Lower baseline amino acid levels such as asparagine and glutamine were correlated with cardiovascular autonomic neuropathy in a small sample of subjects with type 1 diabetes3. Thus, today, it is recognized that the pathogenesis of diabetic peripheral neuropathy is not caused only by abnormal glucose metabolism but is a complex condition in which metabolic failure of other nutrients is involved. However, the full picture of the specific metabolic changes in diabetic peripheral neuropathy has not yet been elucidated.
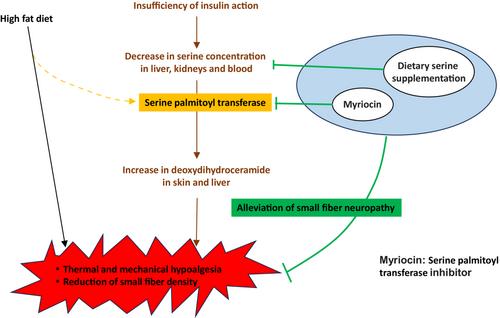
In this context, Handzlik et al.4 recently reported in Nature that the combination of serine deficiency and dyslipidemia can cause experimental diabetic peripheral neuropathy mainly consisting of small fiber neuropathy, in which serine supplementation can delay the onset (Figure 1). The db/db mouse model, which is a conventional obese type 2 diabetic model, showed reductions in hepatic and renal serine levels by approximately 30% relative to wild-type mice, and glycine pools were reduced by 30–50% in the liver, kidney, inguinal white adipose tissue, and plasma. The expression level of components encoding the glycine cleavage system was increased in db/db liver, whereas the expression of genes associated with de novo serine synthesis was significantly reduced. These results indicate that serine synthesis is limited in diabetic mice. Although streptozotocin (STZ)-induced type 1 diabetic model mice showed alterations in plasma glycine and BCAAs (but not serine) at 1 week after streptozotocin treatment, elevated serine disposal was confirmed by co-administration of glucose and serine 2 weeks after injection. Thus, insulin resistance or deficiency can both contribute to the acceleration of serine catabolism or the disposal and reduction of circulating serine in diabetic mice. Of note, weight gain caused by a high-fat diet (HFD) was attenuated by dietary serine and glycine restriction with a reduction in fat mass but not lean mass relative to the treatment with HFD alone, whereas food, calorie, and water intake; calorie absorption; insulin and glucose tolerance; and physical activity were all unaffected. Recent reports suggest that changes in the microbiome composition in the gut can be involved in the pathogenesis of small fiber neuropathy or diabetic peripheral neuropathy5. Investigation of the fecal microbiome revealed that the log ratios of the strains of microorganisms expressing complete serine biosynthesis were increased, while glycine cleavage pathways were decreased with a reduction in the strains expressing a complete fatty acid synthesis pathway by treatment with a serine- and glycine-restricted HFD.
Serine catabolism is associated with sphingolipid metabolism via serine palmitoyl transferase. Sphingolipids are abundantly contained in the myelin sheath in peripheral nerves. Restriction of dietary serine and glycine reduced hepatic palmitate synthesis by approximately 70% relative to serine-replete control diets. Hepatic cholesterol synthesis was increased in the serine-free HFD group compared with the HFD group, with a reduction in the expression of cholesterol biosynthesis enzymes and an increase or no change in the expression of cholesterol biosynthesis enzymes.
Recently, the involvement of insulin resistance in the peripheral nerves has been reported in diabetic peripheral neuropathy, in which proinflammatory macrophage infiltration activated by RAGE signaling elicits deficits in retrograde axonal transportation. Because serine and glycine levels were less associated with changes in protein kinase B phosphorylation than dietary fat and carbohydrate contents, serine restriction could evoke changes in fatty acid metabolism independent of insulin signaling.
Serine deficiency is known to be associated with peripheral neuropathy and various neurodegenerative disorders in previous clinical studies. Similarly, mice fed serine- and glycine-free low-fat chow diets for 12 months exhibited thermal hypoalgesia with intraepidermal nerve fiber reduction in the paw skin. Interestingly, a HFD accelerated the thermal hypoalgesia in mice fed a serine- and glycine-restricted diet for just 3 months. These findings indicate that a combination of low systemic serine and HFD feeding accelerates the onset of small fiber neuropathy in mice. The authors further explored the metabolic changes associated with neuropathy caused by serine restriction. 1-Deoxysphingolipids, including deoxydihydroceramides, are neurotoxic sphingolipids. A 1-deoxysphingolipid is produced when the first enzyme of the sphingolipid biosynthetic pathway, serine palmitoyltransferase, uses l-alanine as a substrate instead of its canonical amino acid substrate, serine. As expected, the contents of deoxydihydro-ceramides in the liver and paw skin increased in serine- and glycine-restricted mice fed HFD, while the canonical ceramide content was reduced. Administration of an inhibitor of serine palmitoyl transferase (myriocin) strongly reduced the levels of sphingolipids as well as of triglycerides and diacylglycerides. Myriocin ameliorated thermal hypoalgesia and the small fiber nerve density in serine- and glycine-restricted HFD mice, while myriocin had no impact on tactile sensing or nerve conduction velocities. Importantly, the administration of myriocin at 6 weeks of age prevented the manifestation of thermal hypoalgesia, tactile sensation, and small fiber density in the epidermis in db/db mice without affecting body weight gain, hyperglycemia, or plasma serine levels. Myriosin treatment strongly reduced canonical sphingolipids in the liver but showed limited effects on paw skin 1-deoxysphingolipids and ceramides. Finally, based on the results obtained thus far, the authors investigated whether a serine-supplemented diet prevents the development of neuropathy. A 3% serine-enriched diet starting at 6 weeks of age elevated levels of plasma and hepatic serine, but not glycine levels. The body weight was comparable, while a slight increase in circulating glucose levels was observed. Neuropathic manifestations, including both thermal and tactile hypoalgesia, were reduced in diabetic mice fed this serine-enriched diet. Canonical sphingolipid levels were similar across the tissues, while 1-deoxysphingolipids were robustly decreased in both liver and paw skin. Collectively, these data suggest that supplementation with serine can prevent the onset and progression of diabetic peripheral neuropathy.
The novel point of this research is that the onset of diabetic peripheral neuropathy could be prevented by correcting the intake of nutrients without affecting blood glucose levels. Currently, no radical therapy for diabetic peripheral neuropathy has been established. Although aldose reductase inhibitors and α-lipoic acid have been clinically applied, their effects are limited. This study suggests that the decrease in serine synthesis and the increase in serine disposal are due to insufficient action of insulin. Although the most important treatment for neuropathy is glycemic control of diabetes itself, it may be necessary to consider treatment of diabetic peripheral neuropathy with a focus on improving insulin action in more organs.
The results of this study also indicate that nutrient factors other than glucose and lipids will accelerate the onset and development of diabetic peripheral neuropathy. This explains one of the reasons why the progression of neuropathy cannot be suppressed by glycemic control alone. Conversely, serine supplementation can prevent the onset of neuropathy to some extent, but not completely in this report. These results reconfirm that diabetic peripheral neuropathy is a multifactorial disease. Therefore, it is conceivable that serine could be administered as an adjunctive therapy in addition to glycemic control.
Unfortunately, the results of this study only relate to the prevention of the onset and progression of experimental diabetic peripheral neuropathy by serine supplementation or myriocin administration, and they do not constitute a treatment. In the future, it will be necessary to evaluate whether correcting serine metabolism can alleviate diabetic peripheral neuropathy that has already developed and progressed or to confirm the efficacy in prospective clinical research.
期刊介绍:
Journal of Diabetes Investigation is your core diabetes journal from Asia; the official journal of the Asian Association for the Study of Diabetes (AASD). The journal publishes original research, country reports, commentaries, reviews, mini-reviews, case reports, letters, as well as editorials and news. Embracing clinical and experimental research in diabetes and related areas, the Journal of Diabetes Investigation includes aspects of prevention, treatment, as well as molecular aspects and pathophysiology. Translational research focused on the exchange of ideas between clinicians and researchers is also welcome. Journal of Diabetes Investigation is indexed by Science Citation Index Expanded (SCIE).



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
