下载PDF
{"title":"Measurements of the Vitamin D Metabolome in the Calgary Vitamin D Study: Relationship of Vitamin D Metabolites to Bone Loss","authors":"Lauren A. Burt, Martin Kaufmann, Marianne S. Rose, Glenville Jones, Emma O. Billington, Steven K. Boyd, David A. Hanley","doi":"10.1002/jbmr.4876","DOIUrl":null,"url":null,"abstract":"<p>In a 36-month randomized controlled trial examining the effect of high-dose vitamin D<sub>3</sub> on radial and tibial total bone mineral density (TtBMD), measured by high-resolution peripheral quantitative tomography (HR-pQCT), participants (311 healthy males and females aged 55–70 years with dual-energy X-ray absorptiometry T-scores > −2.5 without vitamin D deficiency) were randomized to receive 400 IU (<i>N</i> = 109), 4000 IU (<i>N</i> = 100), or 10,000 IU (<i>N</i> = 102) daily. Participants had HR-pQCT radius and tibia scans and blood sampling at baseline, 6, 12, 24, and 36 months. This secondary analysis examined the effect of vitamin D dose on plasma measurements of the vitamin D metabolome by liquid chromatography–tandem mass spectrometry (LC-MS/MS), exploring whether the observed decline in TtBMD was associated with changes in four key metabolites [25-(OH)D<sub>3</sub>; 24,25-(OH)<sub>2</sub>D<sub>3</sub>; 1,25-(OH)<sub>2</sub>D<sub>3</sub>; and 1,24,25-(OH)<sub>3</sub>D<sub>3</sub>]. The relationship between peak values in vitamin D metabolites and changes in TtBMD over 36 months was assessed using linear regression, controlling for sex. Increasing vitamin D dose was associated with a marked increase in 25-(OH)D<sub>3</sub>, 24,25-(OH)<sub>2</sub>D<sub>3</sub> and 1,24,25-(OH)<sub>3</sub>D<sub>3</sub>, but no dose-related change in plasma 1,25-(OH)<sub>2</sub>D<sub>3</sub> was observed. There was a significant negative slope for radius TtBMD and 1,24,25-(OH)<sub>3</sub>D<sub>3</sub> (−0.05, 95% confidence interval [CI] −0.08, −0.03, <i>p</i> < 0.001) after controlling for sex. A significant interaction between TtBMD and sex was seen for 25-(OH)D<sub>3</sub> (female: −0.01, 95% CI −0.12, −0.07; male: −0.04, 95% CI −0.06, −0.01, <i>p</i> = 0.001) and 24,25-(OH)<sub>2</sub>D<sub>3</sub> (female: −0.75, 95% CI −0.98, −0.52; male: −0.35, 95% CI −0.59, −0.11, <i>p</i> < 0.001). For the tibia there was a significant negative slope for 25-(OH)D<sub>3</sub> (−0.03, 95% CI −0.05, −0.01, <i>p</i> < 0.001), 24,25-(OH)<sub>2</sub>D<sub>3</sub> (−0.30, 95% CI −0.44, −0.16, <i>p</i> < 0.001), and 1,24,25-(OH)<sub>3</sub>D<sub>3</sub> (−0.03, 95% CI −0.05, −0.01, <i>p</i> = 0.01) after controlling for sex. These results suggest vitamin D metabolites other than 1,25-(OH)<sub>2</sub>D<sub>3</sub> may be responsible for the bone loss seen in the Calgary Vitamin D Study. Although plasma 1,25-(OH)<sub>2</sub>D<sub>3</sub> did not change with vitamin D dose, it is possible rapid catabolism to 1,24,25-(OH)<sub>3</sub>D<sub>3</sub> prevented the detection of a dose-related rise in plasma 1,25-(OH)<sub>2</sub>D<sub>3</sub>. © 2023 The Authors. <i>Journal of Bone and Mineral Research</i> published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research (ASBMR).</p>","PeriodicalId":185,"journal":{"name":"Journal of Bone and Mineral Research","volume":"38 9","pages":"1312-1321"},"PeriodicalIF":5.9000,"publicationDate":"2023-07-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jbmr.4876","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Mineral Research","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jbmr.4876","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
引用
批量引用
Abstract
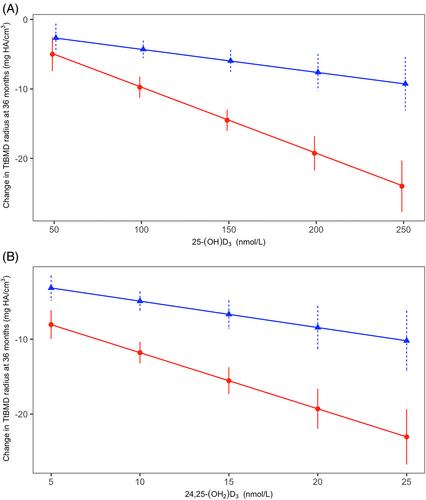
In a 36-month randomized controlled trial examining the effect of high-dose vitamin D3 on radial and tibial total bone mineral density (TtBMD), measured by high-resolution peripheral quantitative tomography (HR-pQCT), participants (311 healthy males and females aged 55–70 years with dual-energy X-ray absorptiometry T-scores > −2.5 without vitamin D deficiency) were randomized to receive 400 IU (N = 109), 4000 IU (N = 100), or 10,000 IU (N = 102) daily. Participants had HR-pQCT radius and tibia scans and blood sampling at baseline, 6, 12, 24, and 36 months. This secondary analysis examined the effect of vitamin D dose on plasma measurements of the vitamin D metabolome by liquid chromatography–tandem mass spectrometry (LC-MS/MS), exploring whether the observed decline in TtBMD was associated with changes in four key metabolites [25-(OH)D3 ; 24,25-(OH)2 D3 ; 1,25-(OH)2 D3 ; and 1,24,25-(OH)3 D3 ]. The relationship between peak values in vitamin D metabolites and changes in TtBMD over 36 months was assessed using linear regression, controlling for sex. Increasing vitamin D dose was associated with a marked increase in 25-(OH)D3 , 24,25-(OH)2 D3 and 1,24,25-(OH)3 D3 , but no dose-related change in plasma 1,25-(OH)2 D3 was observed. There was a significant negative slope for radius TtBMD and 1,24,25-(OH)3 D3 (−0.05, 95% confidence interval [CI] −0.08, −0.03, p < 0.001) after controlling for sex. A significant interaction between TtBMD and sex was seen for 25-(OH)D3 (female: −0.01, 95% CI −0.12, −0.07; male: −0.04, 95% CI −0.06, −0.01, p = 0.001) and 24,25-(OH)2 D3 (female: −0.75, 95% CI −0.98, −0.52; male: −0.35, 95% CI −0.59, −0.11, p < 0.001). For the tibia there was a significant negative slope for 25-(OH)D3 (−0.03, 95% CI −0.05, −0.01, p < 0.001), 24,25-(OH)2 D3 (−0.30, 95% CI −0.44, −0.16, p < 0.001), and 1,24,25-(OH)3 D3 (−0.03, 95% CI −0.05, −0.01, p = 0.01) after controlling for sex. These results suggest vitamin D metabolites other than 1,25-(OH)2 D3 may be responsible for the bone loss seen in the Calgary Vitamin D Study. Although plasma 1,25-(OH)2 D3 did not change with vitamin D dose, it is possible rapid catabolism to 1,24,25-(OH)3 D3 prevented the detection of a dose-related rise in plasma 1,25-(OH)2 D3 . © 2023 The Authors. Journal of Bone and Mineral Research published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research (ASBMR).
卡尔加里维生素D研究中维生素D代谢组的测量:维生素D代谢产物与骨丢失的关系
在一项为期36个月的随机对照试验中,研究了高剂量维生素D3对桡骨和胫骨总骨密度(TtBMD)的影响,通过高分辨率外周定量断层扫描(HR-pQCT)测量,参与者(311名55-70岁的健康男性和女性 双能X射线吸收仪T型芯>;−2.5,无维生素D缺乏)随机接受400 IU(N = 109),4000 IU(N = 100),或10000 IU(N = 102)。参与者在基线、6、12、24和36时进行HR-pQCT桡骨和胫骨扫描和血液采样 月。这项二次分析通过液相色谱-串联质谱法(LC-MS/MS)检测了维生素D剂量对维生素D代谢组血浆测量的影响,探讨了观察到的TtBMD下降是否与四种关键代谢产物[25-(OH)D3;24,25-(OH)2D3;1,25-(OH2D3;和1,24,25-(OH)3D3]的变化有关。维生素D代谢产物峰值与36岁以上TtBMD变化的关系 在控制性别的情况下,采用线性回归法对月数进行评估。维生素D剂量的增加与25-(OH)D3、24,25-(OH)2D3和1,24,25-(OH)3D3的显著增加有关,但未观察到血浆1,25-(OH2D3的剂量相关变化。半径TtBMD和1,24,25-(OH)3D3存在显著的负斜率(−0.05,95%置信区间[CI]−0.08,−0.03,p <; 0.001)。对于25-(OH)D3,TtBMD与性别之间存在显著的相互作用(女性:−0.01,95%CI−0.12,−0.07;男性:−0.04,95%CI−0.06,−0.01,p = 0.001)和24,25-(OH)2D3(雌性:−0.75,95%CI−0.98,−0.52;雄性:−0.35,95%CI–0.59,−0.11,p <; 0.001)。对于胫骨,25-(OH)D3存在显著的负斜率(-0.03,95%CI−0.05,−0.01,p <; 0.001),24,25-(OH)2D3(−0.30,95%CI−0.44,−0.16,p <; 0.001)和1,24,25-(OH)3D3(−0.03,95%CI−0.05,−0.01,p = 0.01)。这些结果表明,除1,25-(OH)2D3外的维生素D代谢产物可能是卡尔加里维生素D研究中发现的骨丢失的原因。尽管血浆1,25-(OH)2D3没有随着维生素D剂量的变化而变化,但对1,24,25-(OH)3D3的快速分解代谢可能阻止了血浆1,25-。©2023作者。由Wiley Periodicals LLC代表美国骨与矿物研究学会(ASBMR)出版的《骨与矿产研究杂志》。
本文章由计算机程序翻译,如有差异,请以英文原文为准。


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
