{"title":"Serum Galectin-3 Predicts Mortality in Venoarterial Extracorporeal Membrane Oxygenation Patients.","authors":"Jianlong Zhu, Dehui Guo, Liying Liu, Jing Zhong","doi":"10.1155/2023/3917156","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We investigated the potential use of galectin-3 (Gal-3) as a prognostic indicator for patients with cardiogenic shock and developed a predictive mortality model for venoarterial extracorporeal membrane oxygenation (VA-ECMO).</p><p><strong>Methods: </strong>We prospectively studied patients (survivors and nonsurvivors) who received VA-ECMO for cardiogenic shock from 2019 to 2021. We recorded baseline data, Gal-3, and B-type natriuretic peptide (BNP) before ECMO and 24-72 h after ECMO. We used multivariable logistic regression to analyze significant risk factors and construct a VA-ECMO death prediction model. Receiver operating characteristic (ROC) curves were plotted to assess the predictive efficacy of the model.</p><p><strong>Results: </strong>We enrolled 73 patients with cardiogenic shock who received VA-ECMO support; 38 (52.05%) died in hospital. The median age was 57 years (interquartile range (IQR): 48-67 years); the median duration of ECMO therapy was 5.8 days (IQR: 4.62-7.57 days); and the median intensive care unit stay was 19.04 days (IQR: 13.92-26.15 days). Compared with the nonsurvivors, survivors had lower acute physiology and chronic health evaluation (APACHE) II scores (<i>p</i> < 0.001), increased left ventricular ejection fraction (<i>p</i> < 0.05), lower Gal-3 levels at 24 and 72 h (both <i>p</i> = 0.001), lower BNP levels at 24 and 72 h (both <i>p</i> = 0.001), and higher platelet counts (<i>p</i> = 0.009). Further multivariable analysis showed that APACHE II score, BNP-T72, and Gal-3-T72 were independent risk factors for death in VA-ECMO patients. Gal-3 and BNP were positively correlated (<i>p</i> < 0.05) and decreased significantly during ECMO treatment. The areas under the ROC curve (AUC) for APACHE II score, Gal-3-T72, and BNP-T72 were 0.687, 0.799, and 0.723, respectively. We constructed a combined prediction model with an AUC of 0.884 (<i>p</i> < 0.01).</p><p><strong>Conclusion: </strong>Gal-3 may serve as a prognostic indicator for patients receiving VA-ECMO for cardiogenic shock. The combined early warning score is a simple and effective tool for predicting mortality in VA-ECMO patients.</p>","PeriodicalId":9494,"journal":{"name":"Cardiology Research and Practice","volume":"2023 ","pages":"3917156"},"PeriodicalIF":1.8000,"publicationDate":"2023-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10560122/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research and Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2023/3917156","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: We investigated the potential use of galectin-3 (Gal-3) as a prognostic indicator for patients with cardiogenic shock and developed a predictive mortality model for venoarterial extracorporeal membrane oxygenation (VA-ECMO).
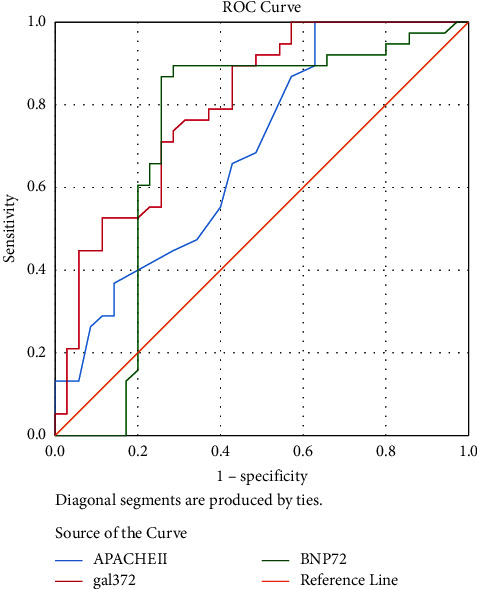
Methods: We prospectively studied patients (survivors and nonsurvivors) who received VA-ECMO for cardiogenic shock from 2019 to 2021. We recorded baseline data, Gal-3, and B-type natriuretic peptide (BNP) before ECMO and 24-72 h after ECMO. We used multivariable logistic regression to analyze significant risk factors and construct a VA-ECMO death prediction model. Receiver operating characteristic (ROC) curves were plotted to assess the predictive efficacy of the model.
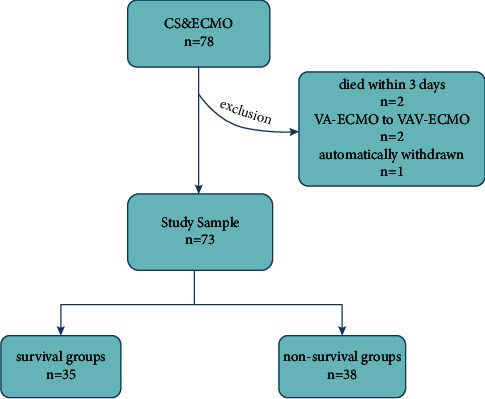
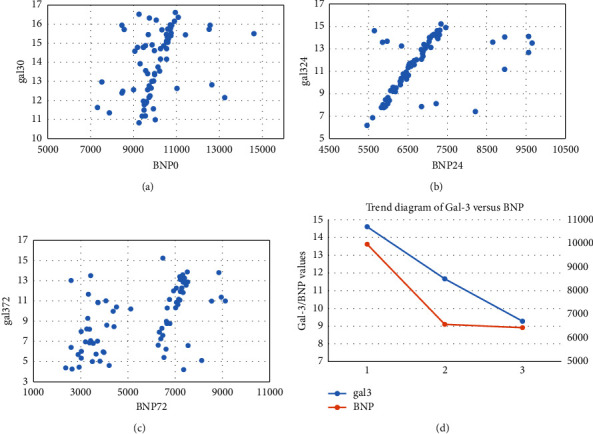
Results: We enrolled 73 patients with cardiogenic shock who received VA-ECMO support; 38 (52.05%) died in hospital. The median age was 57 years (interquartile range (IQR): 48-67 years); the median duration of ECMO therapy was 5.8 days (IQR: 4.62-7.57 days); and the median intensive care unit stay was 19.04 days (IQR: 13.92-26.15 days). Compared with the nonsurvivors, survivors had lower acute physiology and chronic health evaluation (APACHE) II scores (p < 0.001), increased left ventricular ejection fraction (p < 0.05), lower Gal-3 levels at 24 and 72 h (both p = 0.001), lower BNP levels at 24 and 72 h (both p = 0.001), and higher platelet counts (p = 0.009). Further multivariable analysis showed that APACHE II score, BNP-T72, and Gal-3-T72 were independent risk factors for death in VA-ECMO patients. Gal-3 and BNP were positively correlated (p < 0.05) and decreased significantly during ECMO treatment. The areas under the ROC curve (AUC) for APACHE II score, Gal-3-T72, and BNP-T72 were 0.687, 0.799, and 0.723, respectively. We constructed a combined prediction model with an AUC of 0.884 (p < 0.01).
Conclusion: Gal-3 may serve as a prognostic indicator for patients receiving VA-ECMO for cardiogenic shock. The combined early warning score is a simple and effective tool for predicting mortality in VA-ECMO patients.
期刊介绍:
Cardiology Research and Practice is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies that focus on the diagnosis and treatment of cardiovascular disease. The journal welcomes submissions related to systemic hypertension, arrhythmia, congestive heart failure, valvular heart disease, vascular disease, congenital heart disease, and cardiomyopathy.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
