Michelle A Fravel, Calvin J Meaney, Lama Noureddine
{"title":"Management of Hyperkalemia in Patients with Chronic Kidney Disease Using Renin Angiotensin Aldosterone System Inhibitors.","authors":"Michelle A Fravel, Calvin J Meaney, Lama Noureddine","doi":"10.1007/s11906-023-01265-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of review: </strong>Use of renin-angiotensin-aldosterone system (RAAS) inhibiting medications is critical in the prevention of cardiovascular disease and kidney function decline in patients with chronic kidney disease (CKD); however, these agents can lead to hyperkalemia, an electrolyte disorder associated with risk of arrythmia, conduction disorders, and increased overall mortality. Discontinuation, or reduction of dose, of RAAS inhibitor therapy in hyperkalemic patients with CKD can lead to loss of kidney and cardiovascular protection afforded by these medications. Given the high prevalence of hyperkalemia among patients with CKD utilizing RAAS inhibitors, clear management principles are critical to minimize risk and maximize benefit when facing this clinical dilemma.</p><p><strong>Recent findings: </strong>Strategies to mitigate hyperkalemia that do not interfere with optimal RAAS inhibitor therapy should be prioritized when managing potassium elevation in patients with CKD. These strategies include discontinuing non-RAAS inhibitor medications known to cause hyperkalemia, correction of metabolic acidosis, and maximization of medication therapies that lower serum potassium, including diuretics and sodium-glucose cotransporter-2 (SGLT-2) inhibitors. Initiation of potassium exchange resins should also be considered to allow for sustained RAAS inhibitor utilization. An approach which employs multiple strategies concurrently is important to mitigate hyperkalemia and maintain long-term use of RAAS-inhibitors. Persistence of RAAS inhibitor use in patients with CKD is important to slow kidney function decline, delay onset of dialysis or the need for kidney transplant, and prevent adverse cardiovascular outcomes. When hyperkalemia develops among patients with CKD utilizing a RAAS inhibitor, a deliberate effort to reduce serum potassium levels using an approach that allows for continuation of maximally dosed RAAS inhibitor therapy is important. Patient education and engagement in the potassium management process is important for sustained success.</p>","PeriodicalId":10963,"journal":{"name":"Current Hypertension Reports","volume":" ","pages":"395-404"},"PeriodicalIF":5.1000,"publicationDate":"2023-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Hypertension Reports","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11906-023-01265-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/25 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose of review: Use of renin-angiotensin-aldosterone system (RAAS) inhibiting medications is critical in the prevention of cardiovascular disease and kidney function decline in patients with chronic kidney disease (CKD); however, these agents can lead to hyperkalemia, an electrolyte disorder associated with risk of arrythmia, conduction disorders, and increased overall mortality. Discontinuation, or reduction of dose, of RAAS inhibitor therapy in hyperkalemic patients with CKD can lead to loss of kidney and cardiovascular protection afforded by these medications. Given the high prevalence of hyperkalemia among patients with CKD utilizing RAAS inhibitors, clear management principles are critical to minimize risk and maximize benefit when facing this clinical dilemma.
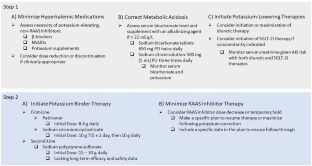
Recent findings: Strategies to mitigate hyperkalemia that do not interfere with optimal RAAS inhibitor therapy should be prioritized when managing potassium elevation in patients with CKD. These strategies include discontinuing non-RAAS inhibitor medications known to cause hyperkalemia, correction of metabolic acidosis, and maximization of medication therapies that lower serum potassium, including diuretics and sodium-glucose cotransporter-2 (SGLT-2) inhibitors. Initiation of potassium exchange resins should also be considered to allow for sustained RAAS inhibitor utilization. An approach which employs multiple strategies concurrently is important to mitigate hyperkalemia and maintain long-term use of RAAS-inhibitors. Persistence of RAAS inhibitor use in patients with CKD is important to slow kidney function decline, delay onset of dialysis or the need for kidney transplant, and prevent adverse cardiovascular outcomes. When hyperkalemia develops among patients with CKD utilizing a RAAS inhibitor, a deliberate effort to reduce serum potassium levels using an approach that allows for continuation of maximally dosed RAAS inhibitor therapy is important. Patient education and engagement in the potassium management process is important for sustained success.
期刊介绍:
This journal intends to provide clear, insightful, balanced contributions by international experts that review the most important, recently published clinical findings related to the diagnosis, treatment, management, and prevention of hypertension.
We accomplish this aim by appointing international authorities to serve as Section Editors in key subject areas, such as antihypertensive therapies, associated metabolic disorders, and therapeutic trials. Section Editors, in turn, select topics for which leading experts contribute comprehensive review articles that emphasize new developments and recently published papers of major importance, highlighted by annotated reference lists. An international Editorial Board reviews the annual table of contents, suggests articles of special interest to their country/region, and ensures that topics are current and include emerging research. Commentaries from well-known figures in the field are also provided.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
