{"title":"Endocortical Trabecularization in Acromegaly: The Cause for the Paradoxically Increased Vertebral Fracture Risk?","authors":"Ansgar Heck, Kristin Godang, Tove Lekva, Kjersti Norman Markussen, Sara De Vincentis, Thor Ueland, Jens Bollerslev","doi":"10.1002/jbm4.10787","DOIUrl":null,"url":null,"abstract":"<p>Growth hormone (GH) is nonphysiologically increased in acromegaly, stimulating target tissues directly and indirectly via insulin-like growth factor type 1 (IGF-1). Despite GH having anabolic effects on bone growth and renewal, the risk of vertebral fractures is paradoxically increased in acromegaly. We hypothesized that bone tissue compartments were differentially affected by hormonal alterations in active and controlled acromegaly. We aimed to study the effect of sex and gonadal status on long-term outcome of bone mass and structure to understand the biomechanical competence of bone. We followed 62 patients with newly diagnosed acromegaly longitudinally (median 4.8 years after pituitary surgery) to investigate changes assessed by dual X-ray absorptiometry (DXA), trabecular bone score (TBS), and hip structure analysis (HSA). At diagnosis, patients had increased bone mineral density (BMD) in most compartments compared with normative data (Z-scores). Conversely, TBS Z-score was decreased (Z = −0.64 (SD 1.73), <i>p</i> = 0.028). Following treatment of acromegaly, BMD increased further in compartments containing predominantly trabecular bone, such as the lumbar spine, in eugonadal and male subjects, while compartments with predominantly cortical bone, such as the hip and femoral neck, were unchanged. Total body measurements showed further increase in BMD independent of sex and gonadal status. TBS did not change. HSA revealed a significant decrease in cortical thickness in both sexes independent of gonadal status, whereas the overall size of bone (hip axis length and neck width) did not change over time. In conclusion, patients with acromegaly had increased bone mass and dimensions by DXA. Following normalization of disease activity, BMD increased mainly in compartments rich in trabecular bone, reflecting a closure of the remodeling space. However, HSA revealed a significant decrease in cortical thickness, implying endocortical trabecularization, potentially explaining the increased risk for incident vertebral fractures following treatment. © 2023 The Authors. <i>JBMR Plus</i> published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research.</p>","PeriodicalId":14611,"journal":{"name":"JBMR Plus","volume":"7 10","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2023-08-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://asbmr.onlinelibrary.wiley.com/doi/epdf/10.1002/jbm4.10787","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBMR Plus","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jbm4.10787","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
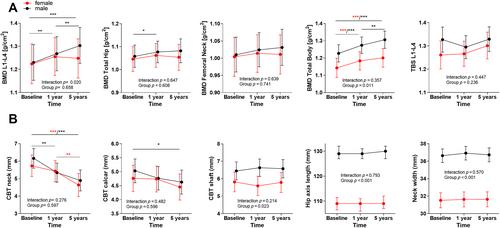
Growth hormone (GH) is nonphysiologically increased in acromegaly, stimulating target tissues directly and indirectly via insulin-like growth factor type 1 (IGF-1). Despite GH having anabolic effects on bone growth and renewal, the risk of vertebral fractures is paradoxically increased in acromegaly. We hypothesized that bone tissue compartments were differentially affected by hormonal alterations in active and controlled acromegaly. We aimed to study the effect of sex and gonadal status on long-term outcome of bone mass and structure to understand the biomechanical competence of bone. We followed 62 patients with newly diagnosed acromegaly longitudinally (median 4.8 years after pituitary surgery) to investigate changes assessed by dual X-ray absorptiometry (DXA), trabecular bone score (TBS), and hip structure analysis (HSA). At diagnosis, patients had increased bone mineral density (BMD) in most compartments compared with normative data (Z-scores). Conversely, TBS Z-score was decreased (Z = −0.64 (SD 1.73), p = 0.028). Following treatment of acromegaly, BMD increased further in compartments containing predominantly trabecular bone, such as the lumbar spine, in eugonadal and male subjects, while compartments with predominantly cortical bone, such as the hip and femoral neck, were unchanged. Total body measurements showed further increase in BMD independent of sex and gonadal status. TBS did not change. HSA revealed a significant decrease in cortical thickness in both sexes independent of gonadal status, whereas the overall size of bone (hip axis length and neck width) did not change over time. In conclusion, patients with acromegaly had increased bone mass and dimensions by DXA. Following normalization of disease activity, BMD increased mainly in compartments rich in trabecular bone, reflecting a closure of the remodeling space. However, HSA revealed a significant decrease in cortical thickness, implying endocortical trabecularization, potentially explaining the increased risk for incident vertebral fractures following treatment. © 2023 The Authors. JBMR Plus published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research.
肢端肥大症的皮质内小梁化:脊椎骨折风险异常增加的原因?
生长激素(GH)在肢端肥大症中非生理性增加,通过胰岛素样生长因子1型(IGF-1)直接或间接刺激靶组织。尽管生长激素对骨骼生长和更新有合成代谢作用,但肢端肥大症的脊椎骨折风险却增加了。我们假设,活动性肢端肥大症和对照性肢端肥大的骨组织区室受到激素改变的不同影响。我们旨在研究性别和性腺状态对骨量和结构的长期结果的影响,以了解骨骼的生物力学能力。我们对62名新诊断的肢端肥大症患者进行了纵向随访(中位数4.8 垂体手术后数年),以研究通过双X射线吸收仪(DXA)、骨小梁评分(TBS)和髋关节结构分析(HSA)评估的变化。在诊断时,与标准数据(Z评分)相比,患者大多数区域的骨密度(BMD)增加。相反,TBS Z评分降低(Z = -0.64(标准差1.73),p = 0.028)。肢端肥大症治疗后,在性腺正常和男性受试者中,主要含有小梁骨的区域(如腰椎)的BMD进一步增加,而主要含有皮质骨的区域,如髋关节和股骨颈,则没有变化。全身测量显示BMD进一步增加,与性别和性腺状态无关。TBS没有改变。HSA显示,与性腺状态无关,两性的皮质厚度都显著降低,而骨骼的总体大小(髋轴长度和颈部宽度)没有随时间变化。总之,通过DXA,肢端肥大症患者的骨量和骨尺寸增加。疾病活动正常化后,BMD主要在富含小梁骨的区域增加,反映出重塑空间的闭合。然而,HSA显示皮质厚度显著降低,这意味着皮质内小梁化,这可能解释了治疗后发生脊椎骨折的风险增加。©2023作者。由Wiley Periodicals LLC代表美国骨与矿物研究学会出版的JBMR Plus。
本文章由计算机程序翻译,如有差异,请以英文原文为准。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
