Omid Ghaemi, Mohammad-Mehdi Mehrabi Nejad, Mohammad Reza Rouhezamin, Niloofar Ayoobi Yazdi, Ramin Pourghorban, Hadi Rokni Yazdi
{"title":"A technical review of percutaneous sclerotherapy with bleomycin for giant hepatic venous malformation.","authors":"Omid Ghaemi, Mohammad-Mehdi Mehrabi Nejad, Mohammad Reza Rouhezamin, Niloofar Ayoobi Yazdi, Ramin Pourghorban, Hadi Rokni Yazdi","doi":"10.1186/s42155-023-00394-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hepatic venous malformation (HVM), traditionally called liver haemangioma, is considered the most common benign hepatic lesion. Treatment might be indicated in large and symptomatic HVMs. We aim to describe stepwise technical aspects of trans-hepatic percutaneous sclerotherapy of hepatic venous malformation (HVM).</p><p><strong>Main text: </strong>Patients with symptomatic HVM larger than 5 cm are selected after discussion in hepatobiliary multidisciplinary team. After prophylactic antibiotic and corticosteroid administration, local anaesthesia and conscious sedation are applied. A 22-gauge spinal or Chiba needle is used to obtain percutaneous access to the HVM through normal liver parenchyma under ultrasound guidance. To ensure proper needle placement and to prevent accidental delivery of sclerosant into unintended areas, about 5-10 mL iodine contrast is injected under fluoroscopy. Then, 45-60 IU bleomycin is mixed with 10 mL distilled water and 10 mL lipiodol and is slowly injected under fluoroscopy over a period of 20-30 s. After the needle is removed, manual pressure is applied over the puncture site for a period of 5 min followed by placement of a sandbag. Patients are monitored for 6-8 h post-procedure.</p><p><strong>Conclusion: </strong>In this technical review, we described our institutional technique of percutaneous sclerotherapy, which could be regarded as an alternative to TAE in the management of HVM.</p>","PeriodicalId":52351,"journal":{"name":"CVIR Endovascular","volume":"6 1","pages":"46"},"PeriodicalIF":1.5000,"publicationDate":"2023-09-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10533756/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CVIR Endovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42155-023-00394-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Hepatic venous malformation (HVM), traditionally called liver haemangioma, is considered the most common benign hepatic lesion. Treatment might be indicated in large and symptomatic HVMs. We aim to describe stepwise technical aspects of trans-hepatic percutaneous sclerotherapy of hepatic venous malformation (HVM).
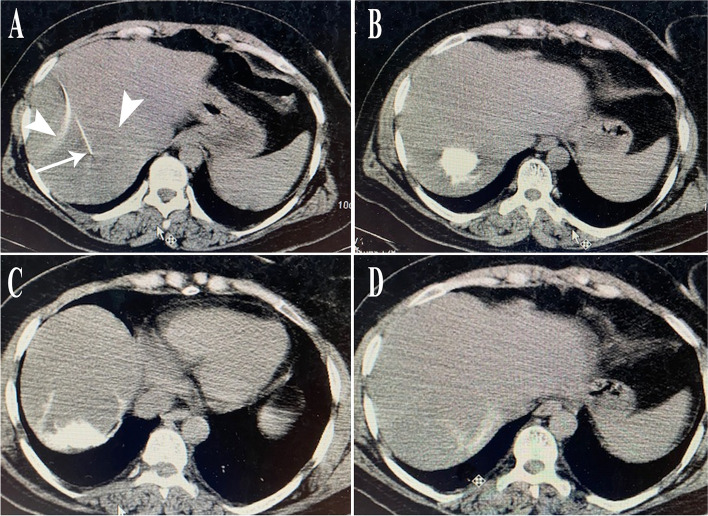
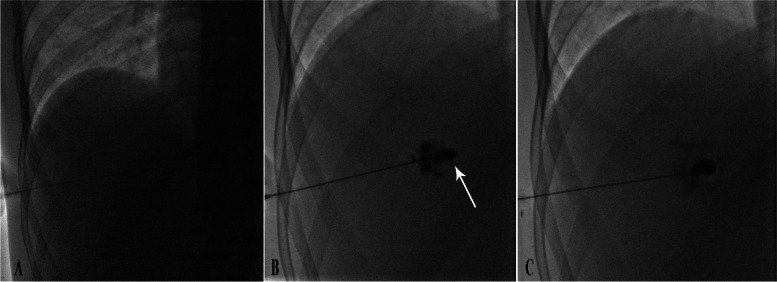
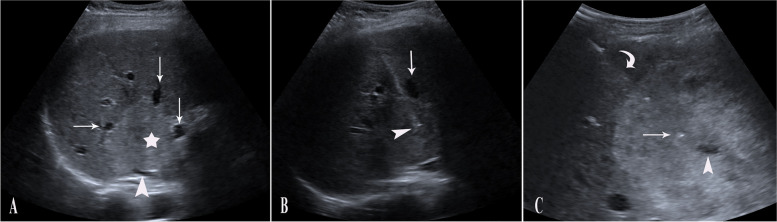
Main text: Patients with symptomatic HVM larger than 5 cm are selected after discussion in hepatobiliary multidisciplinary team. After prophylactic antibiotic and corticosteroid administration, local anaesthesia and conscious sedation are applied. A 22-gauge spinal or Chiba needle is used to obtain percutaneous access to the HVM through normal liver parenchyma under ultrasound guidance. To ensure proper needle placement and to prevent accidental delivery of sclerosant into unintended areas, about 5-10 mL iodine contrast is injected under fluoroscopy. Then, 45-60 IU bleomycin is mixed with 10 mL distilled water and 10 mL lipiodol and is slowly injected under fluoroscopy over a period of 20-30 s. After the needle is removed, manual pressure is applied over the puncture site for a period of 5 min followed by placement of a sandbag. Patients are monitored for 6-8 h post-procedure.
Conclusion: In this technical review, we described our institutional technique of percutaneous sclerotherapy, which could be regarded as an alternative to TAE in the management of HVM.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
