Leon J. Wils, Jos B. Poell, Laura A. N. Peferoen, Ilkay Evren, Elisabeth R. Brouns, Jan G. A. M. de Visscher, Erik H. van der Meij, Ruud H. Brakenhoff, Elisabeth Bloemena
{"title":"The role of differentiated dysplasia in the prediction of malignant transformation of oral leukoplakia","authors":"Leon J. Wils, Jos B. Poell, Laura A. N. Peferoen, Ilkay Evren, Elisabeth R. Brouns, Jan G. A. M. de Visscher, Erik H. van der Meij, Ruud H. Brakenhoff, Elisabeth Bloemena","doi":"10.1111/jop.13483","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>Oral leukoplakia is the most common oral potentially malignant disorder. Malignant transformation of oral leukoplakia occurs at an annual rate of 1%–7%. WHO-defined classic epithelial dysplasia is an important predictor of malignant transformation of oral leukoplakia, but we have previously shown in a proof of concept study that prediction improves by incorporation of an architectural pattern of dysplasia, also coined as differentiated dysplasia. We aimed to analyze this finding in a larger cohort of patients.</p>\n </section>\n \n <section>\n \n <h3> Method</h3>\n \n <p>For this retrospective study 176 oral leukoplakia patients were included. Biopsies for all patients were assessed for the presence of dysplasia and analyzed for cytokeratin 13 and 17 expression. Moreover, the inter-observer agreement for the diagnosis of differentiated dysplasia was determined.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>In total, 33 of 176 patients developed oral squamous cell carcinoma during follow-up. Presence of classic epithelial dysplasia increased cancer risk two-fold (HR = 2.18, <i>p</i> = 0.026). Lesions without classic epithelial dysplasia could be further risk-stratified by the presence of differentiated dysplasia (HR = 7.36, <i>p</i> < 0.001). Combined classic epithelial and differentiated dysplasia imparted a seven-fold increased risk of malignant transformation (7.34, <i>p</i> = 0.001). Inter-observer agreement for the diagnosis of dysplasia, including differentiated dysplasia, was moderate (κ = 0.56, <i>p</i> < 0.001).</p>\n </section>\n \n <section>\n \n <h3> Discussion</h3>\n \n <p>This study emphasizes the importance of the recognition of the architectural pattern of differentiated dysplasia as a separate entity for risk prediction of malignant transformation of oral leukoplakia. Presence of any pattern of dysplasia results in accurate prediction of malignant transformation risk of oral leukoplakia.</p>\n </section>\n </div>","PeriodicalId":16588,"journal":{"name":"Journal of Oral Pathology & Medicine","volume":"52 10","pages":"930-938"},"PeriodicalIF":2.3000,"publicationDate":"2023-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jop.13483","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Oral Pathology & Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jop.13483","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
Oral leukoplakia is the most common oral potentially malignant disorder. Malignant transformation of oral leukoplakia occurs at an annual rate of 1%–7%. WHO-defined classic epithelial dysplasia is an important predictor of malignant transformation of oral leukoplakia, but we have previously shown in a proof of concept study that prediction improves by incorporation of an architectural pattern of dysplasia, also coined as differentiated dysplasia. We aimed to analyze this finding in a larger cohort of patients.
Method
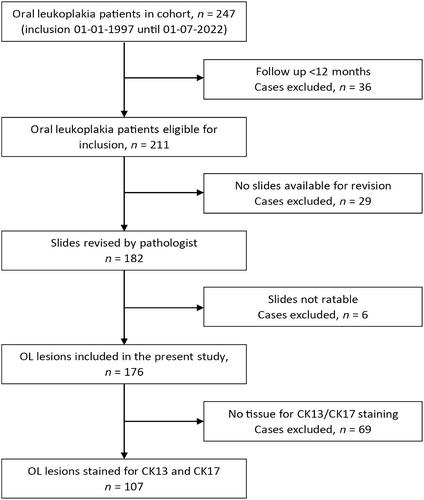
For this retrospective study 176 oral leukoplakia patients were included. Biopsies for all patients were assessed for the presence of dysplasia and analyzed for cytokeratin 13 and 17 expression. Moreover, the inter-observer agreement for the diagnosis of differentiated dysplasia was determined.
Results
In total, 33 of 176 patients developed oral squamous cell carcinoma during follow-up. Presence of classic epithelial dysplasia increased cancer risk two-fold (HR = 2.18, p = 0.026). Lesions without classic epithelial dysplasia could be further risk-stratified by the presence of differentiated dysplasia (HR = 7.36, p < 0.001). Combined classic epithelial and differentiated dysplasia imparted a seven-fold increased risk of malignant transformation (7.34, p = 0.001). Inter-observer agreement for the diagnosis of dysplasia, including differentiated dysplasia, was moderate (κ = 0.56, p < 0.001).
Discussion
This study emphasizes the importance of the recognition of the architectural pattern of differentiated dysplasia as a separate entity for risk prediction of malignant transformation of oral leukoplakia. Presence of any pattern of dysplasia results in accurate prediction of malignant transformation risk of oral leukoplakia.
期刊介绍:
The aim of the Journal of Oral Pathology & Medicine is to publish manuscripts of high scientific quality representing original clinical, diagnostic or experimental work in oral pathology and oral medicine. Papers advancing the science or practice of these disciplines will be welcomed, especially those which bring new knowledge and observations from the application of techniques within the spheres of light and electron microscopy, tissue and organ culture, immunology, histochemistry and immunocytochemistry, microbiology, genetics and biochemistry.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
