{"title":"Ureter Injury in Laparoscopic Para-Aortic Lymphadenectomy for Endometrial Cancer by the Transperitoneal Approach.","authors":"Hiroharu Kobayashi, Misa Kobayashi, Yoshihiro Takaki, Yuki Kondo, Yuri Hamada, Haruhiko Shimizu, Yumi Shimizu, Masaru Nagashima, Hiroshi Adachi","doi":"10.1155/2023/3138683","DOIUrl":null,"url":null,"abstract":"<p><p>The patient was 66 years old, had three pregnancies and two deliveries, and was menopausal at the age of 51. She had irregular bleeding and was found to have a chicken-egg-sized uterus and a thickened endometrium (23 mm). She underwent laparoscopic surgery for uterine endometrial cancer (endometrioid carcinoma G1, stage IB). Laparoscopic simple hysterectomy, bilateral adnexectomy, pelvic lymph node dissection, para-aortic lymph node dissection, and partial omentectomy were performed using the transperitoneal approach (TPA). The patient was obese, with a height of 148 cm, a weight of 68 kg, and a body mass index of 31 kg/m<sup>2</sup>. She had a large amount of visceral fat, which made it difficult to expand the surgical field during para-aortic lymph node dissection. A laparoscopic fan retractor (EndoRetract II, Medtronic) was used to lift the intestinal tracts and expand the field of view. It broke the fat around the left kidney, and the exposed left ureter was heat-damaged using a vessel sealing device (LigaSure, Medtronic). Postoperatively, a left ureteral stent was placed, and continuous urine draining into the retroperitoneum was performed. To prevent injury to the left ureter, the left ovarian vein branching from the left renal vein should be exposed as a landmark before the left ureter running parallel to it is isolated. It is essential that the fat around the left kidney is not broken during this operation. The left iliopsoas muscle should be exposed, and using this as a base, the left ovarian vein, left ureter, and left perirenal fat should be compressed and moved to the left side using a fan retractor to ensure a safe operation.</p>","PeriodicalId":9610,"journal":{"name":"Case Reports in Obstetrics and Gynecology","volume":"2023 ","pages":"3138683"},"PeriodicalIF":0.8000,"publicationDate":"2023-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10522427/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Obstetrics and Gynecology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/3138683","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
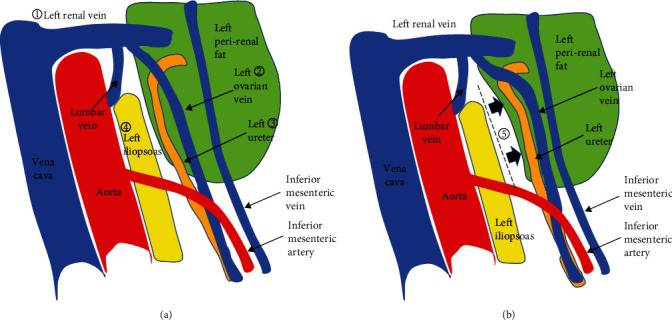
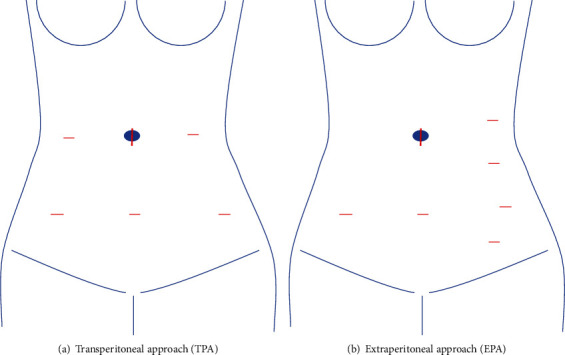
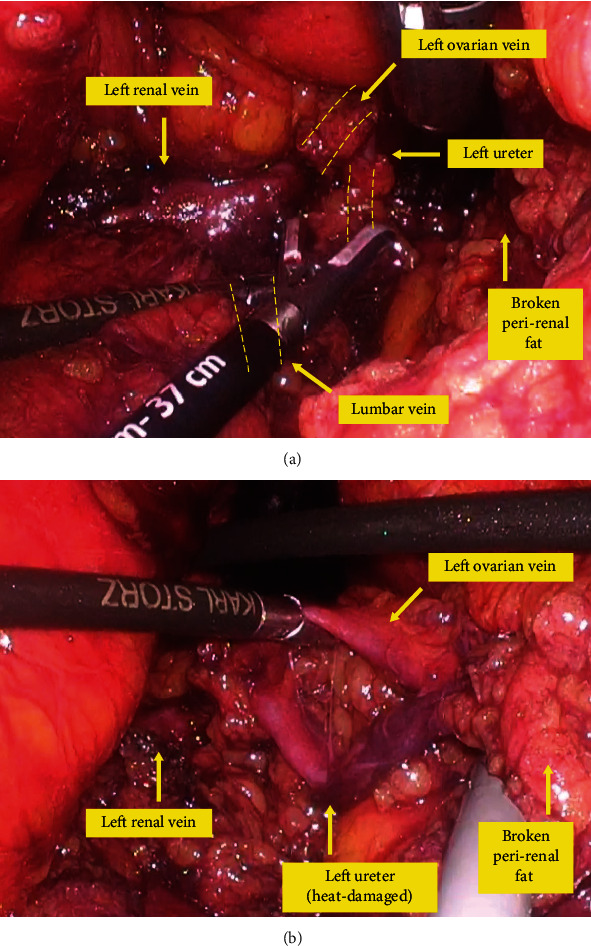
The patient was 66 years old, had three pregnancies and two deliveries, and was menopausal at the age of 51. She had irregular bleeding and was found to have a chicken-egg-sized uterus and a thickened endometrium (23 mm). She underwent laparoscopic surgery for uterine endometrial cancer (endometrioid carcinoma G1, stage IB). Laparoscopic simple hysterectomy, bilateral adnexectomy, pelvic lymph node dissection, para-aortic lymph node dissection, and partial omentectomy were performed using the transperitoneal approach (TPA). The patient was obese, with a height of 148 cm, a weight of 68 kg, and a body mass index of 31 kg/m2. She had a large amount of visceral fat, which made it difficult to expand the surgical field during para-aortic lymph node dissection. A laparoscopic fan retractor (EndoRetract II, Medtronic) was used to lift the intestinal tracts and expand the field of view. It broke the fat around the left kidney, and the exposed left ureter was heat-damaged using a vessel sealing device (LigaSure, Medtronic). Postoperatively, a left ureteral stent was placed, and continuous urine draining into the retroperitoneum was performed. To prevent injury to the left ureter, the left ovarian vein branching from the left renal vein should be exposed as a landmark before the left ureter running parallel to it is isolated. It is essential that the fat around the left kidney is not broken during this operation. The left iliopsoas muscle should be exposed, and using this as a base, the left ovarian vein, left ureter, and left perirenal fat should be compressed and moved to the left side using a fan retractor to ensure a safe operation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
