{"title":"Whether it is safe to start anticoagulation after intracranial hemorrhage within 2 weeks: A systematic review and meta-analysis","authors":"Xue-Yan Huang, Jun-Yan Zhang, Chang-Yin Yu","doi":"10.1002/ibra.12060","DOIUrl":null,"url":null,"abstract":"<p>Whether restarting anticoagulation (RA) treatment after intracranial hemorrhage (ICH) is still controversial. We performed a systematic review and meta-analysis to summarize the relationship between anticoagulation after ICH with the recurrence of hemorrhagic events, ischemic events, and long-term mortality. Medline, Embase, and the Cochrane Central Register of Controlled Trials, from inception to November 2020. We searched the published medical literature to ensure cohort studies involving ICH associated with anticoagulation in adults. Primary outcomes were long-term mortality, hemorrhagic events, and ischemic events (myocardial infarction, pulmonary embolism, ischemic stroke, or systemic embolization). We concluded seven retrospective cohorts, including 1876 intracranial hemorrhage patients with indications of anticoagulation. The ratio of the anticoagulant restart was 35.3% (664n). RA was associated with a significantly lower incidence of recurrent ischemic events (pooled odds ratio [OR] 0.29, 95% confidence interval [CI] 0.19% to 0.45%, <i>p</i> = 0.97) and death events (pooled OR 0.56, 95% CI 0.40%–0.79%, <i>p</i> = 0.27). There is no evidence that early recovery of anticoagulation (within 2 weeks or 1 month) is associated with the occurrence of hemorrhagic events (within 2 weeks: pooled OR 0.80, 95% CI 0.3–2.12, <i>p</i> = 0.52 vs. within 1 month: pooled OR 1.14, 95% CI 0.77–1.68, <i>p</i> = 0.82). Based on these, recovery of anticoagulation after ICH is beneficial for long-term mortality and recurrence of ischemic events. The meta-analysis showed a resumption of oral anticoagulation within 2 weeks or 1 month in patients who had a cerebral hemorrhage was beneficial and did not increase the risk of hemorrhagic events and reduced the occurrence of ischemic and fatal endpoint events.</p>","PeriodicalId":94030,"journal":{"name":"Ibrain","volume":"8 3","pages":"377-388"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10528763/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ibrain","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ibra.12060","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
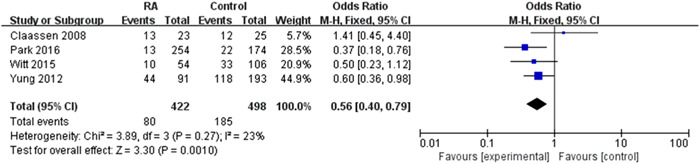
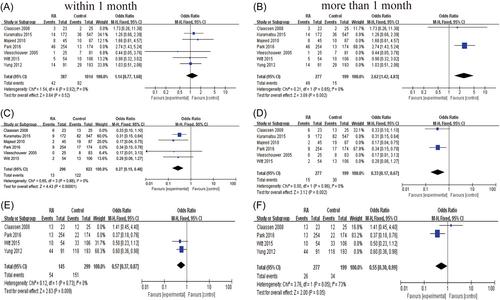
Whether restarting anticoagulation (RA) treatment after intracranial hemorrhage (ICH) is still controversial. We performed a systematic review and meta-analysis to summarize the relationship between anticoagulation after ICH with the recurrence of hemorrhagic events, ischemic events, and long-term mortality. Medline, Embase, and the Cochrane Central Register of Controlled Trials, from inception to November 2020. We searched the published medical literature to ensure cohort studies involving ICH associated with anticoagulation in adults. Primary outcomes were long-term mortality, hemorrhagic events, and ischemic events (myocardial infarction, pulmonary embolism, ischemic stroke, or systemic embolization). We concluded seven retrospective cohorts, including 1876 intracranial hemorrhage patients with indications of anticoagulation. The ratio of the anticoagulant restart was 35.3% (664n). RA was associated with a significantly lower incidence of recurrent ischemic events (pooled odds ratio [OR] 0.29, 95% confidence interval [CI] 0.19% to 0.45%, p = 0.97) and death events (pooled OR 0.56, 95% CI 0.40%–0.79%, p = 0.27). There is no evidence that early recovery of anticoagulation (within 2 weeks or 1 month) is associated with the occurrence of hemorrhagic events (within 2 weeks: pooled OR 0.80, 95% CI 0.3–2.12, p = 0.52 vs. within 1 month: pooled OR 1.14, 95% CI 0.77–1.68, p = 0.82). Based on these, recovery of anticoagulation after ICH is beneficial for long-term mortality and recurrence of ischemic events. The meta-analysis showed a resumption of oral anticoagulation within 2 weeks or 1 month in patients who had a cerebral hemorrhage was beneficial and did not increase the risk of hemorrhagic events and reduced the occurrence of ischemic and fatal endpoint events.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
