Joanna Magdalena Tomasiuk, Anna Nowakowska-Płaza, Małgorzata Wisłowska, Piotr Głuszko
{"title":"Osteoporosis and diabetes - possible links and diagnostic difficulties.","authors":"Joanna Magdalena Tomasiuk, Anna Nowakowska-Płaza, Małgorzata Wisłowska, Piotr Głuszko","doi":"10.5114/reum/170048","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>In this review, the authors aimed to clarify the relationship between the occurrence of osteoporosis and diabetes, analyze the differences between the pathogenesis of osteoporosis in different types of diabetes and propose the most effective diagnostic strategy and fracture risk assessment in diabetic patients.</p><p><strong>Material and methods: </strong>A analysis of publications in MEDLINE, COCHRANE and SCOPUS databases was performed, searching for reports on the diagnostics, fracture risk assessment, prevention, and treatment of osteoporosis in patients with diabetes mellitus (DM) published in the years 2016-2022. The key words for the search were: diabetes, osteoporosis, and low-energy fracture.</p><p><strong>Results: </strong>Bone complications of T1DM are more severe than T2DM, because of the lack of anabolic effect of insulin on bones. In T2DM the risk of fractures is elevated; however, identifying the mechanisms underlying the increased risk of fractures in T2DM is not clear. The FRAX tool is not appropriate for assessing the fracture risk in young patients with T1DM. It is quite useful in older patients with T2DM, but in these patients the calculated fracture risk may be underestimated. In T2DM the fracture risk often does not correspond to BMD value as measured by dual-energy X-ray absorptiometry (DXA). Diagnostic tools such as the trabecular bone score may play a significant role in this group of patients. Conclusions: Optimal strategies to identify and treat high risk individuals require further research and proper definition. The diagnostic criteria for osteoporosis should be clearly defined as well as fracture risk assessment and choice of anti-osteoporotic medication. In all cases of secondary osteoporosis, treatment of the underlying disease is the most important. The relationship between high risk of fractures and diabetes is inseparable, and its full understanding seems to be the key to effective management.</p>","PeriodicalId":21312,"journal":{"name":"Reumatologia","volume":"61 4","pages":"294-304"},"PeriodicalIF":1.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3f/ba/RU-61-170048.PMC10515121.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reumatologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/reum/170048","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/3 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: In this review, the authors aimed to clarify the relationship between the occurrence of osteoporosis and diabetes, analyze the differences between the pathogenesis of osteoporosis in different types of diabetes and propose the most effective diagnostic strategy and fracture risk assessment in diabetic patients.
Material and methods: A analysis of publications in MEDLINE, COCHRANE and SCOPUS databases was performed, searching for reports on the diagnostics, fracture risk assessment, prevention, and treatment of osteoporosis in patients with diabetes mellitus (DM) published in the years 2016-2022. The key words for the search were: diabetes, osteoporosis, and low-energy fracture.
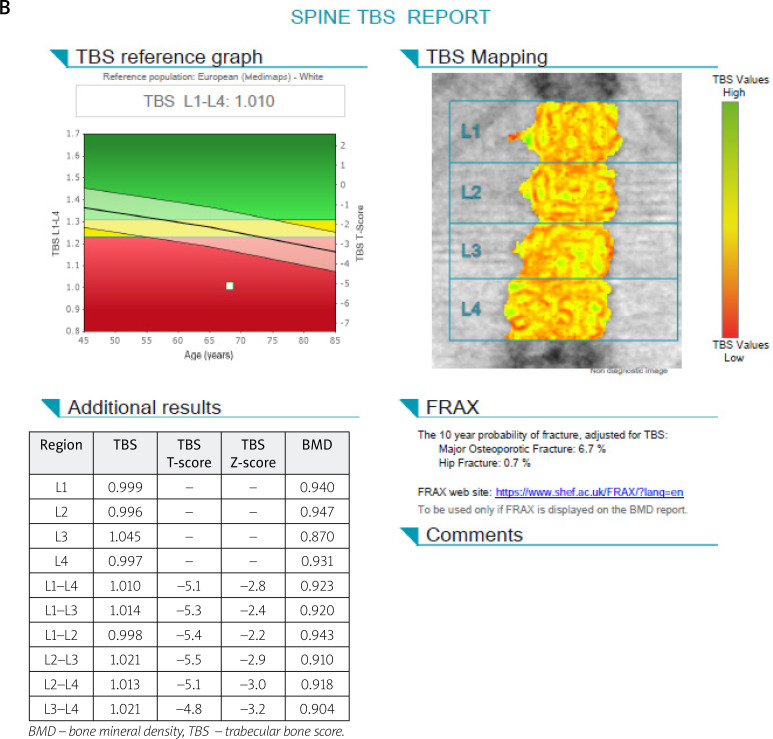
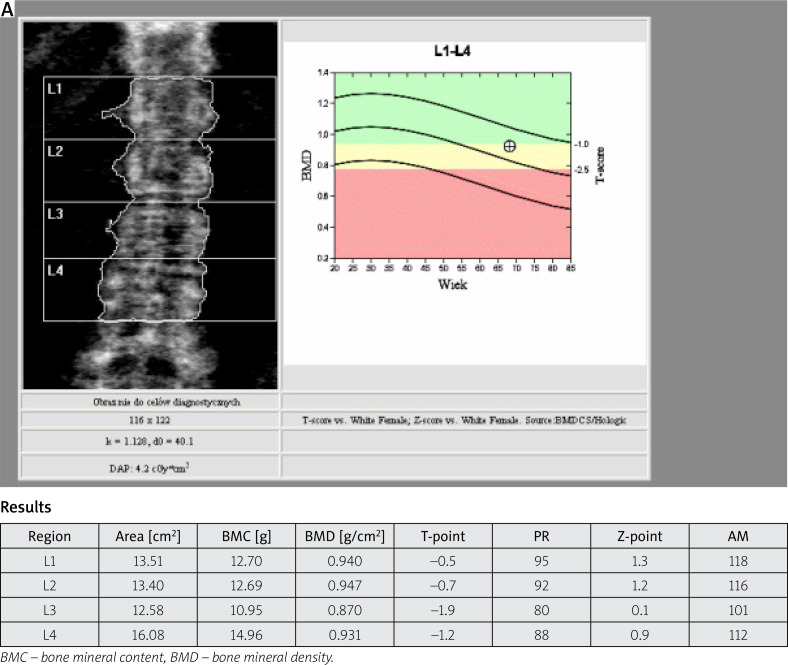
Results: Bone complications of T1DM are more severe than T2DM, because of the lack of anabolic effect of insulin on bones. In T2DM the risk of fractures is elevated; however, identifying the mechanisms underlying the increased risk of fractures in T2DM is not clear. The FRAX tool is not appropriate for assessing the fracture risk in young patients with T1DM. It is quite useful in older patients with T2DM, but in these patients the calculated fracture risk may be underestimated. In T2DM the fracture risk often does not correspond to BMD value as measured by dual-energy X-ray absorptiometry (DXA). Diagnostic tools such as the trabecular bone score may play a significant role in this group of patients. Conclusions: Optimal strategies to identify and treat high risk individuals require further research and proper definition. The diagnostic criteria for osteoporosis should be clearly defined as well as fracture risk assessment and choice of anti-osteoporotic medication. In all cases of secondary osteoporosis, treatment of the underlying disease is the most important. The relationship between high risk of fractures and diabetes is inseparable, and its full understanding seems to be the key to effective management.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
