William Vainchenker, Nasrine Yahmi, Violaine Havelange, Caroline Marty, Isabelle Plo, Stefan N Constantinescu
{"title":"Recent advances in therapies for primary myelofibrosis.","authors":"William Vainchenker, Nasrine Yahmi, Violaine Havelange, Caroline Marty, Isabelle Plo, Stefan N Constantinescu","doi":"10.12703/r/12-23","DOIUrl":null,"url":null,"abstract":"<p><p>Primary myelofibrosis (PMF), polycythemia vera (PV) and essential thrombocythemia (ET) form the classical <i>BCR-ABL1</i>-negative myeloproliferative neoplasms (MPNs) that are driven by a constitutive activation of JAK2 signaling. PMF as well as secondary MF (post-ET and post-PV MF) are the most aggressive MPNs. Presently, there is no curative treatment, except allogenic hematopoietic stem cell transplantation. JAK inhibitors, essentially ruxolitinib, are the therapy of reference for intermediate and high-risk MF. However, presently the current JAK inhibitors behave mainly as anti-inflammatory drugs, improving general symptoms and spleen size without major impact on disease progression. A better understanding of the genetics of MF, the biology of its leukemic stem cells (LSCs), the mechanisms of fibrosis and of cytopenia and the role of inflammatory cytokines has led to new approaches with the development of numerous therapeutic agents that target epigenetic regulation, telomerase, apoptosis, cell cycle, cytokines and signaling. Furthermore, the use of a new less toxic form of interferon-α has been revived, as it is presently one of the only molecules that targets the mutated clone. These new approaches have different aims: (a) to provide alternative therapy to JAK inhibition; (b) to correct cytopenia; and (c) to inhibit fibrosis development. However, the main important goal is to find new disease modifier treatments, which will profoundly modify the progression of the disease without major toxicity. Presently the most promising approaches consist of the inhibition of telomerase and the combination of JAK2 inhibitors (ruxolitinib) with either a BCL2/BCL-xL or BET inhibitor. Yet, the most straightforward future approaches can be considered to be the development of and/or selective inhibition of JAK2V617F and the targeting MPL and calreticulin mutants by immunotherapy. It can be expected that the therapy of MF will be significantly improved in the coming years.</p>","PeriodicalId":73016,"journal":{"name":"Faculty reviews","volume":"12 ","pages":"23"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10523375/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Faculty reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12703/r/12-23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
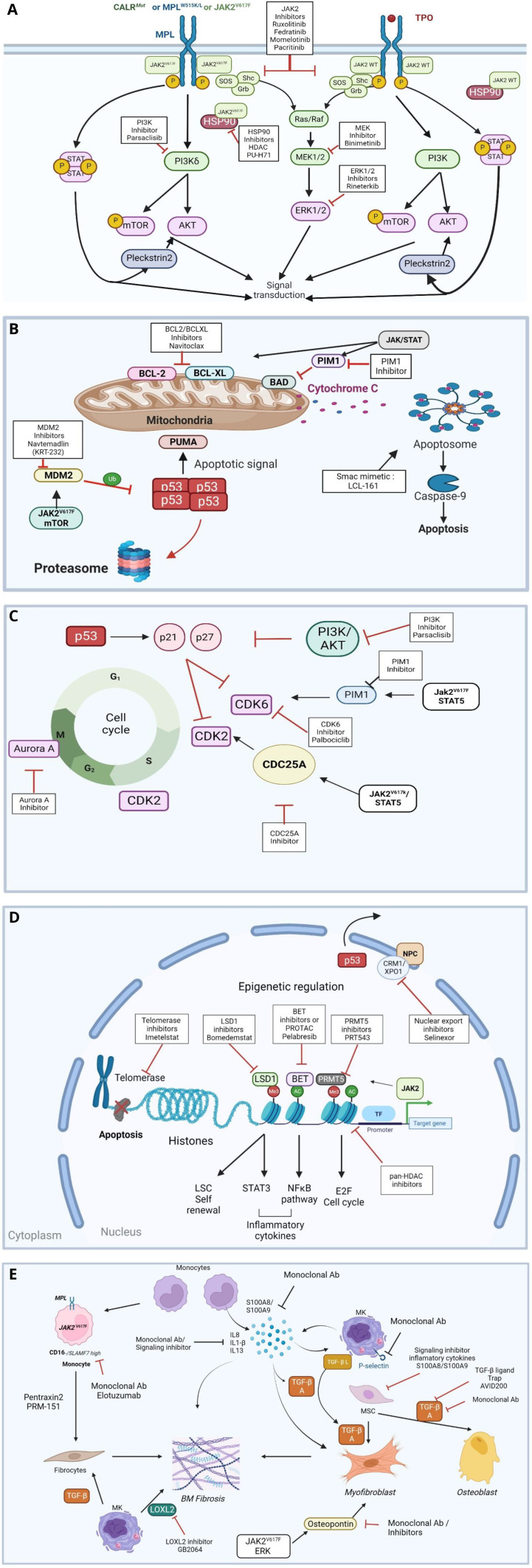
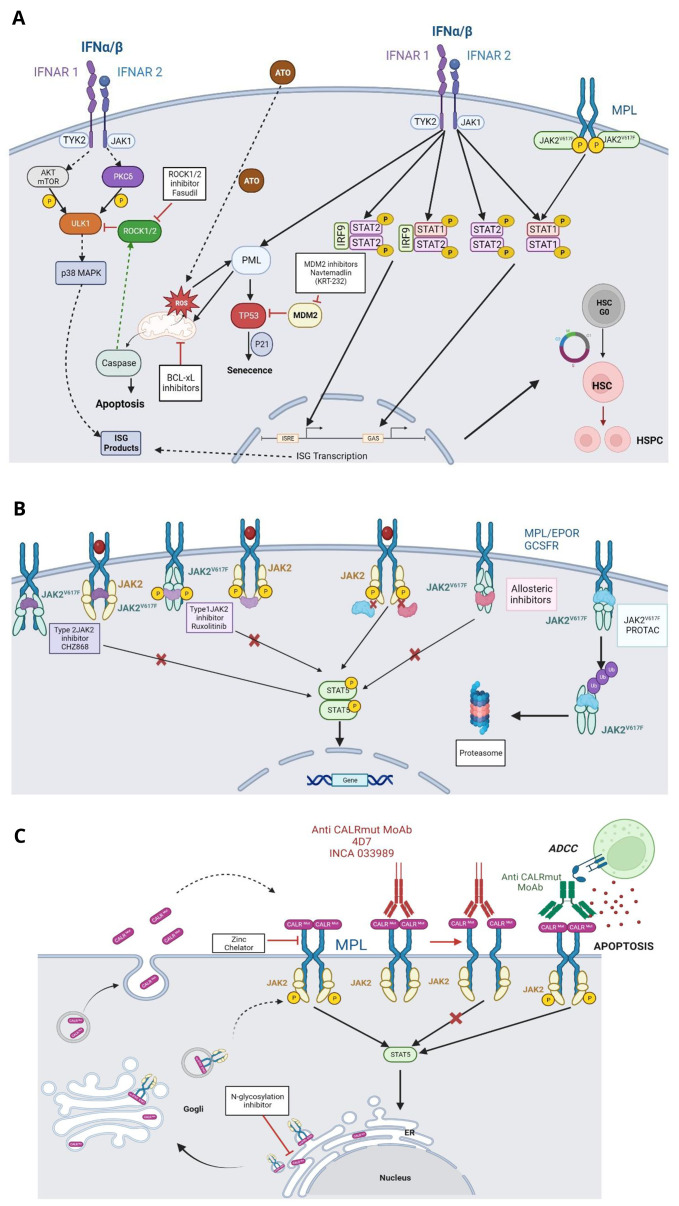
Primary myelofibrosis (PMF), polycythemia vera (PV) and essential thrombocythemia (ET) form the classical BCR-ABL1-negative myeloproliferative neoplasms (MPNs) that are driven by a constitutive activation of JAK2 signaling. PMF as well as secondary MF (post-ET and post-PV MF) are the most aggressive MPNs. Presently, there is no curative treatment, except allogenic hematopoietic stem cell transplantation. JAK inhibitors, essentially ruxolitinib, are the therapy of reference for intermediate and high-risk MF. However, presently the current JAK inhibitors behave mainly as anti-inflammatory drugs, improving general symptoms and spleen size without major impact on disease progression. A better understanding of the genetics of MF, the biology of its leukemic stem cells (LSCs), the mechanisms of fibrosis and of cytopenia and the role of inflammatory cytokines has led to new approaches with the development of numerous therapeutic agents that target epigenetic regulation, telomerase, apoptosis, cell cycle, cytokines and signaling. Furthermore, the use of a new less toxic form of interferon-α has been revived, as it is presently one of the only molecules that targets the mutated clone. These new approaches have different aims: (a) to provide alternative therapy to JAK inhibition; (b) to correct cytopenia; and (c) to inhibit fibrosis development. However, the main important goal is to find new disease modifier treatments, which will profoundly modify the progression of the disease without major toxicity. Presently the most promising approaches consist of the inhibition of telomerase and the combination of JAK2 inhibitors (ruxolitinib) with either a BCL2/BCL-xL or BET inhibitor. Yet, the most straightforward future approaches can be considered to be the development of and/or selective inhibition of JAK2V617F and the targeting MPL and calreticulin mutants by immunotherapy. It can be expected that the therapy of MF will be significantly improved in the coming years.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
