Using information technology to integrate tobacco use treatment in routine oncology care: Lessons learned from the U.S. Cancer Center Cessation Initiative Cancer Centers.
Jennifer E Bird, Claire Vt Nguyen, Sarah D Hohl, Heather D'Angelo, Danielle Pauk, Robert T Adsit, Michael Fiore, Mara Minion, Danielle McCarthy, Betsy Rolland
{"title":"Using information technology to integrate tobacco use treatment in routine oncology care: Lessons learned from the U.S. Cancer Center Cessation Initiative Cancer Centers.","authors":"Jennifer E Bird, Claire Vt Nguyen, Sarah D Hohl, Heather D'Angelo, Danielle Pauk, Robert T Adsit, Michael Fiore, Mara Minion, Danielle McCarthy, Betsy Rolland","doi":"10.1177/26334895231185374","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cancer patients who receive evidence-based tobacco-dependence treatment are more likely to quit and remain abstinent, but tobacco treatment programs (TTPs) are not consistently offered. In 2017, the U.S. National Cancer Institute, through the Cancer Moonshot, funded the Cancer Center Cessation Initiative (C3I). C3I supports 52 cancer centers to implement and expand evidence-based tobacco treatment in routine oncology care. Integration into routine care involves the use of health information technology (IT), including modifying electronic health records and clinical workflows. Here, we examine C3I cancer centers' IT leadership involvement and experiences in tobacco-dependence treatment implementation.</p><p><strong>Method: </strong>This qualitative study of C3I-funded cancer centers integrated data from online surveys and in-person, semistructured interviews with IT leaders. We calculated descriptive statistics of survey data and applied content analysis to interview transcripts.</p><p><strong>Results: </strong>Themes regarding IT personnel included suggestions to involve IT early, communicate regularly, understand the roles and influence of the IT team, and match program design with IT funding and resources. Themes regarding electronic health record (EHR) modifications included beginning modifications early to account for long lead time to make changes, working with IT to identify and adapt existing EHR tools for TTP or designing tools that will support a desired workflow developed with end-users, and working with IT personnel to make sure TTPs comply with system and state policies (e.g., privacy laws).</p><p><strong>Conclusions: </strong>The experiences of C3I cancer centers regarding the use of health IT to enhance tobacco-dependence treatment program implementation can guide cancer centers and community oncology practices to potentially enhance TTP implementation and patient outcomes.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"4 ","pages":"26334895231185374"},"PeriodicalIF":2.6000,"publicationDate":"2023-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b0/e7/10.1177_26334895231185374.PMC10331328.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895231185374","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
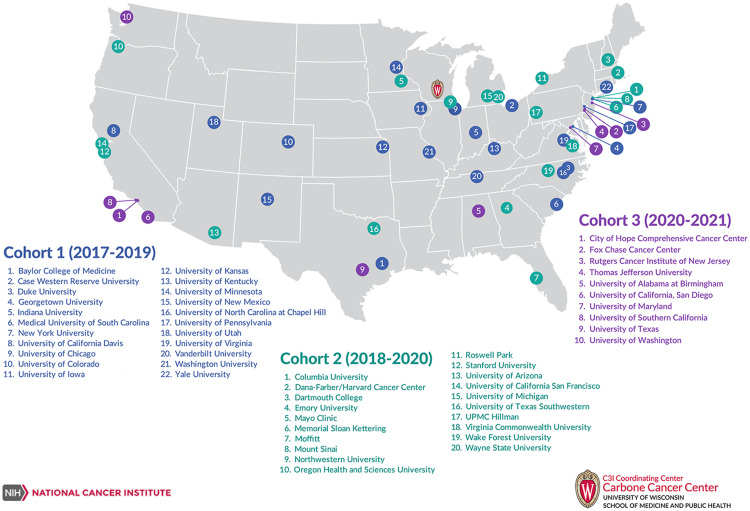
Background: Cancer patients who receive evidence-based tobacco-dependence treatment are more likely to quit and remain abstinent, but tobacco treatment programs (TTPs) are not consistently offered. In 2017, the U.S. National Cancer Institute, through the Cancer Moonshot, funded the Cancer Center Cessation Initiative (C3I). C3I supports 52 cancer centers to implement and expand evidence-based tobacco treatment in routine oncology care. Integration into routine care involves the use of health information technology (IT), including modifying electronic health records and clinical workflows. Here, we examine C3I cancer centers' IT leadership involvement and experiences in tobacco-dependence treatment implementation.
Method: This qualitative study of C3I-funded cancer centers integrated data from online surveys and in-person, semistructured interviews with IT leaders. We calculated descriptive statistics of survey data and applied content analysis to interview transcripts.
Results: Themes regarding IT personnel included suggestions to involve IT early, communicate regularly, understand the roles and influence of the IT team, and match program design with IT funding and resources. Themes regarding electronic health record (EHR) modifications included beginning modifications early to account for long lead time to make changes, working with IT to identify and adapt existing EHR tools for TTP or designing tools that will support a desired workflow developed with end-users, and working with IT personnel to make sure TTPs comply with system and state policies (e.g., privacy laws).
Conclusions: The experiences of C3I cancer centers regarding the use of health IT to enhance tobacco-dependence treatment program implementation can guide cancer centers and community oncology practices to potentially enhance TTP implementation and patient outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
