Christina Köhler, Luise Tittl, Ulrike Hänsel, Evelyn Hammermüller, Sandra Marten, Christiane Naue, Marianne Spindler, Laura Stannek, Kristina Fache, Jan Beyer-Westendorf
{"title":"Periinterventional Management of Edoxaban in Major Procedures: Results from the DRESDEN NOAC REGISTRY.","authors":"Christina Köhler, Luise Tittl, Ulrike Hänsel, Evelyn Hammermüller, Sandra Marten, Christiane Naue, Marianne Spindler, Laura Stannek, Kristina Fache, Jan Beyer-Westendorf","doi":"10.1055/s-0043-1774304","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b> Edoxaban is a non-vitamin K dependent oral anticoagulant (NOAC) licensed for venous thromboembolism (VTE) treatment or stroke prevention in atrial fibrillation. Major surgical procedures are not uncommon in anticoagulated patients but data on perioperative edoxaban management are scarce. <b>Patients and Methods</b> Using data from the prospective DRESDEN NOAC REGISTRY, we extracted data on major surgical procedures in edoxaban patients. Periinterventional edoxaban management patterns and rates of outcome events were evaluated until day 30 after procedure. <b>Results</b> Between 2011 and 2021, 3,448 procedures were identified in edoxaban patients, including 287 (8.3%) major procedures. A scheduled interruption of edoxaban was observed in 284/287 major procedures (99%) with a total median edoxaban interruption time of 11.0 days (25-75th percentile: 5.0-18.0 days). Heparin bridging was documented in 183 procedures (46 prophylactic dosages, 111 intermediate and 26 therapeutic dosages). Overall, 7 (2.4%; 95% CI: 1.2-4.9%) major cardiovascular events (5 VTE, 2 arterial thromboembolic events) and 38 major bleedings (13.2%; 95% CI: 9.8-17.7%) were observed and 6 patients died (2.1%; 95% CI: 1.0-4.5%). Rates of major cardiovascular events with or without heparin bridging were comparable (4/137; 2.9%; 95% CI: 1.1-7.3% vs. 3/82; 3.7%; 95% CI: 1.3-10.2%). Major bleedings occurred numerically more frequent in patients receiving heparin bridging (23/137; 16.8%; 95% CI: 11.5-23.9%) versus procedures without heparin bridging (9/82; 11.0%; 95% CI: 5.9-19.6%). <b>Conclusion</b> Within the limitations of our study design, real-world periprocedural edoxaban management seems effective and safe. Use of heparin bridging seems to have limited effects on reducing vascular events but may increase bleeding risk.</p>","PeriodicalId":94220,"journal":{"name":"TH open : companion journal to thrombosis and haemostasis","volume":"7 3","pages":"e251-e261"},"PeriodicalIF":1.8000,"publicationDate":"2023-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10516686/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"TH open : companion journal to thrombosis and haemostasis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1774304","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
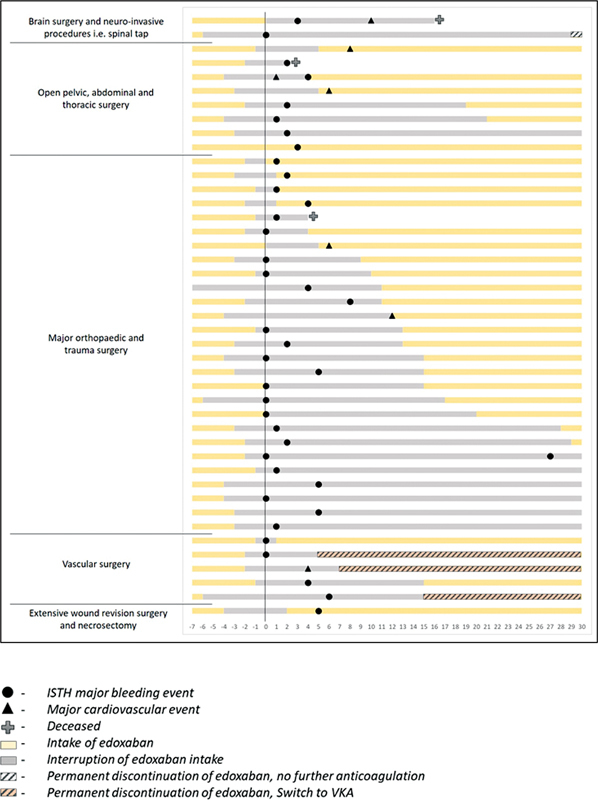
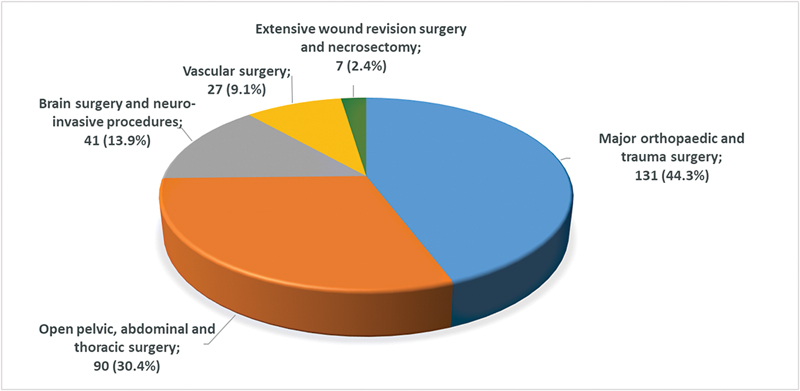
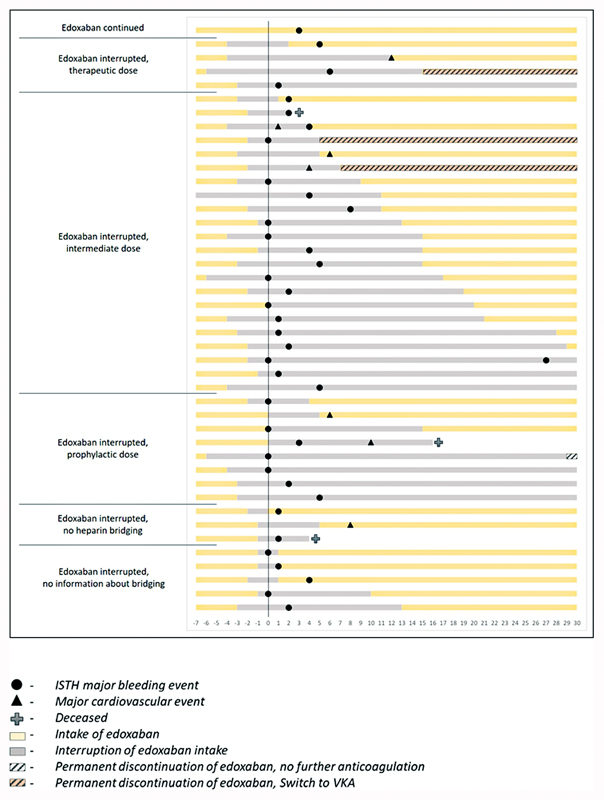
Background Edoxaban is a non-vitamin K dependent oral anticoagulant (NOAC) licensed for venous thromboembolism (VTE) treatment or stroke prevention in atrial fibrillation. Major surgical procedures are not uncommon in anticoagulated patients but data on perioperative edoxaban management are scarce. Patients and Methods Using data from the prospective DRESDEN NOAC REGISTRY, we extracted data on major surgical procedures in edoxaban patients. Periinterventional edoxaban management patterns and rates of outcome events were evaluated until day 30 after procedure. Results Between 2011 and 2021, 3,448 procedures were identified in edoxaban patients, including 287 (8.3%) major procedures. A scheduled interruption of edoxaban was observed in 284/287 major procedures (99%) with a total median edoxaban interruption time of 11.0 days (25-75th percentile: 5.0-18.0 days). Heparin bridging was documented in 183 procedures (46 prophylactic dosages, 111 intermediate and 26 therapeutic dosages). Overall, 7 (2.4%; 95% CI: 1.2-4.9%) major cardiovascular events (5 VTE, 2 arterial thromboembolic events) and 38 major bleedings (13.2%; 95% CI: 9.8-17.7%) were observed and 6 patients died (2.1%; 95% CI: 1.0-4.5%). Rates of major cardiovascular events with or without heparin bridging were comparable (4/137; 2.9%; 95% CI: 1.1-7.3% vs. 3/82; 3.7%; 95% CI: 1.3-10.2%). Major bleedings occurred numerically more frequent in patients receiving heparin bridging (23/137; 16.8%; 95% CI: 11.5-23.9%) versus procedures without heparin bridging (9/82; 11.0%; 95% CI: 5.9-19.6%). Conclusion Within the limitations of our study design, real-world periprocedural edoxaban management seems effective and safe. Use of heparin bridging seems to have limited effects on reducing vascular events but may increase bleeding risk.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
