Hyeonsik Kim, Hyun-Kyu Yoon, Hyeonhoon Lee, Chul-Woo Jung, Hyung-Chul Lee
{"title":"Predicting optimal endotracheal tube size and depth in pediatric patients using demographic data and machine learning techniques.","authors":"Hyeonsik Kim, Hyun-Kyu Yoon, Hyeonhoon Lee, Chul-Woo Jung, Hyung-Chul Lee","doi":"10.4097/kja.23501","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Use of endotracheal tubes (ETTs) with appropriate size and depth can help minimize intubation-related complications in pediatric patients. Existing age-based formulae for selecting the optimal ETT size present several inaccuracies. We developed a machine learning model that predicts the optimal size and depth of ETTs in pediatric patients using demographic data, enabling clinical applications.</p><p><strong>Methods: </strong>Data from 37,057 patients younger than 12 years who underwent general anesthesia with endotracheal intubation were retrospectively analyzed. Gradient boosted regression tree (GBRT) model was developed and compared with traditional age-based formulae.</p><p><strong>Results: </strong>The GBRT model demonstrated the highest macro-averaged F1 scores of 0.502 (95% CI 0.486, 0.568) and 0.669 (95% CI 0.640, 0.694) for predicting the uncuffed and cuffed ETT size (internal diameter [ID]), outperforming the age-based formulae that yielded 0.163 (95% CI 0.140, 0.196, P < 0.001) and 0.392 (95% CI 0.378, 0.406, P < 0.001), respectively. In predicting the ETT depth (distance from tip to lip corner), the GBRT model showed the lowest mean absolute error (MAE) of 0.71 cm (95% CI 0.69, 0.72) and 0.72 cm (95% CI 0.70, 0.74) compared to the age-based formulae that showed an error of 1.18 cm (95% CI 1.16, 1.20, P < 0.001) and 1.34 cm (95% CI 1.31, 1.38, P < 0.001) for uncuffed and cuffed ETT, respectively.</p><p><strong>Conclusions: </strong>The GBRT model using only demographic data accurately predicted the ETT size and depth. If these results are validated, the model may be practical for predicting optimal ETT size and depth for pediatric patients.</p>","PeriodicalId":17855,"journal":{"name":"Korean Journal of Anesthesiology","volume":" ","pages":"540-549"},"PeriodicalIF":6.3000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10718635/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Anesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4097/kja.23501","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/26 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Use of endotracheal tubes (ETTs) with appropriate size and depth can help minimize intubation-related complications in pediatric patients. Existing age-based formulae for selecting the optimal ETT size present several inaccuracies. We developed a machine learning model that predicts the optimal size and depth of ETTs in pediatric patients using demographic data, enabling clinical applications.
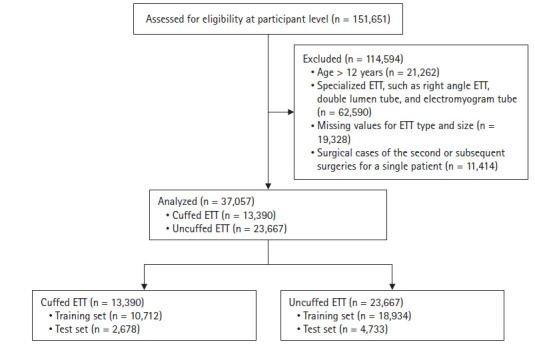
Methods: Data from 37,057 patients younger than 12 years who underwent general anesthesia with endotracheal intubation were retrospectively analyzed. Gradient boosted regression tree (GBRT) model was developed and compared with traditional age-based formulae.
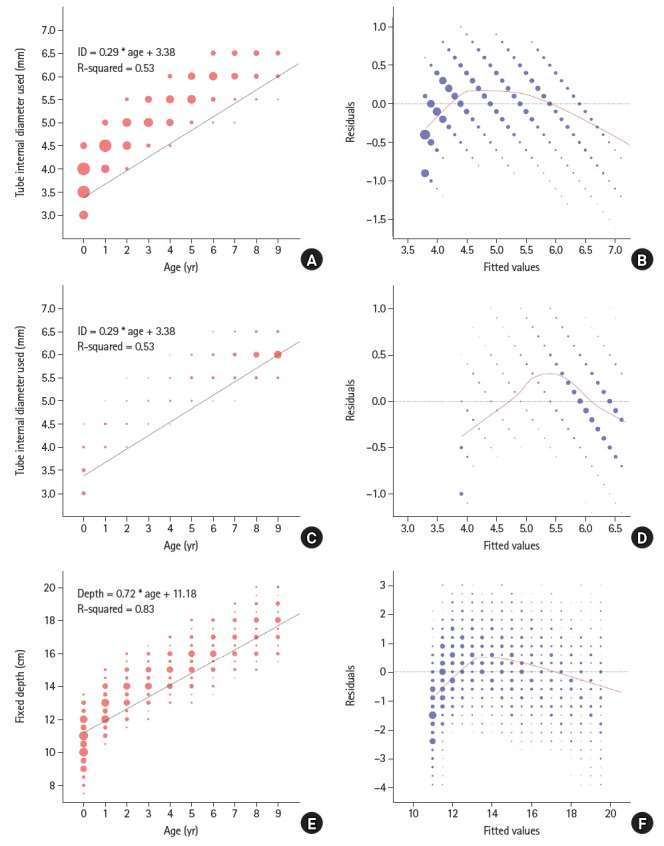
Results: The GBRT model demonstrated the highest macro-averaged F1 scores of 0.502 (95% CI 0.486, 0.568) and 0.669 (95% CI 0.640, 0.694) for predicting the uncuffed and cuffed ETT size (internal diameter [ID]), outperforming the age-based formulae that yielded 0.163 (95% CI 0.140, 0.196, P < 0.001) and 0.392 (95% CI 0.378, 0.406, P < 0.001), respectively. In predicting the ETT depth (distance from tip to lip corner), the GBRT model showed the lowest mean absolute error (MAE) of 0.71 cm (95% CI 0.69, 0.72) and 0.72 cm (95% CI 0.70, 0.74) compared to the age-based formulae that showed an error of 1.18 cm (95% CI 1.16, 1.20, P < 0.001) and 1.34 cm (95% CI 1.31, 1.38, P < 0.001) for uncuffed and cuffed ETT, respectively.
Conclusions: The GBRT model using only demographic data accurately predicted the ETT size and depth. If these results are validated, the model may be practical for predicting optimal ETT size and depth for pediatric patients.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
