{"title":"Geographic disparities persist despite decline in mortality from IHD in California's Central Valley 1999-2014.","authors":"Ralph Spada, Nicholas Spada, Hyosim Seon-Spada","doi":"10.1177/2048004019866320","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Nationally, ischemic heart disease mortality has declined significantly due to advancements in managing traditional risk factors of hypertension, diabetes, hyperlipidemia, smoking, and obesity and acute intervention. However geographic disparities persist that may, in part, be attributed to environmental effects.</p><p><strong>Methods: </strong>Ischemic heart disease age-adjusted mortality were obtained from the CDC database for years 1999 through 2014 by county, gender, race, and Hispanic origin for the Central Valley of California.</p><p><strong>Results: </strong>There was an increase in mortality from north to south of 14.9 (95% CI: 8.0-21.9, p value <0.0001) in time period 1, 7.9 (95% CI: 0.8-15, p value <0.05) in time period 2, and 9.2 (95% CI: 4.0-14.3, p value <0.001) in time period 3. In time period 1, the ambient particulate matter ≤2.5 micrometers (PM<sub>2.5</sub>) level increased from north to south by 0.84 µg/m³ (95% CI: 0.71-0.96), in time period 2 there was a 0.87 µg/m³ increase (95% CI: 0.74-1.0), and a 1.0 µg/m³ increase in time period 3 (95% CI: 0.87-1.1). PM<sub>2.5</sub> level was correlated to IHD mortality in all time periods (Period 1 r<sup>2</sup> = 0.46, p = 0.0001; Period 2, r<sup>2</sup> = 0.34, p = 0.008; Period 3 r<sup>2</sup> = 0.51, p value <0.0001).</p><p><strong>Conclusion: </strong>Continued declines in ischemic heart disease mortality will depend on the concerted efforts of clinicians in continuing management of the traditional risk factors with appropriate medication use, acute interventions for coronary syndromes, the necessity of patient self-management of high risk behaviors associated with smoking and obesity, and the development of coordinated actions with policy makers to reduce environmental exposure in their respective communities.</p>","PeriodicalId":30457,"journal":{"name":"JRSM Cardiovascular Disease","volume":"8 ","pages":"2048004019866320"},"PeriodicalIF":1.5000,"publicationDate":"2019-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2048004019866320","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JRSM Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2048004019866320","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
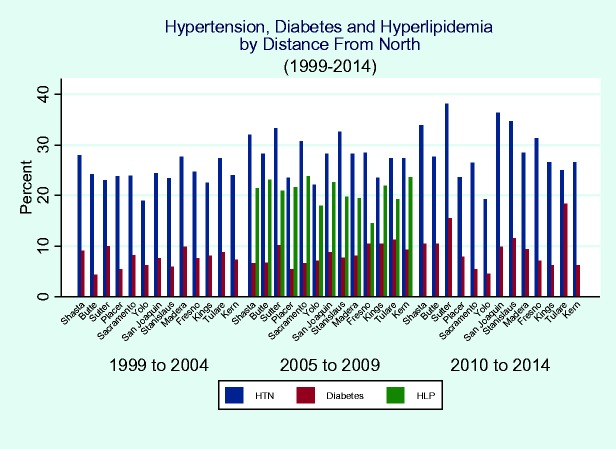
Background: Nationally, ischemic heart disease mortality has declined significantly due to advancements in managing traditional risk factors of hypertension, diabetes, hyperlipidemia, smoking, and obesity and acute intervention. However geographic disparities persist that may, in part, be attributed to environmental effects.
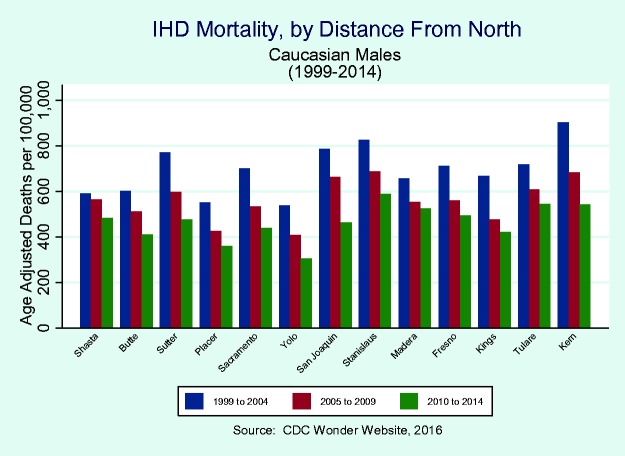
Methods: Ischemic heart disease age-adjusted mortality were obtained from the CDC database for years 1999 through 2014 by county, gender, race, and Hispanic origin for the Central Valley of California.
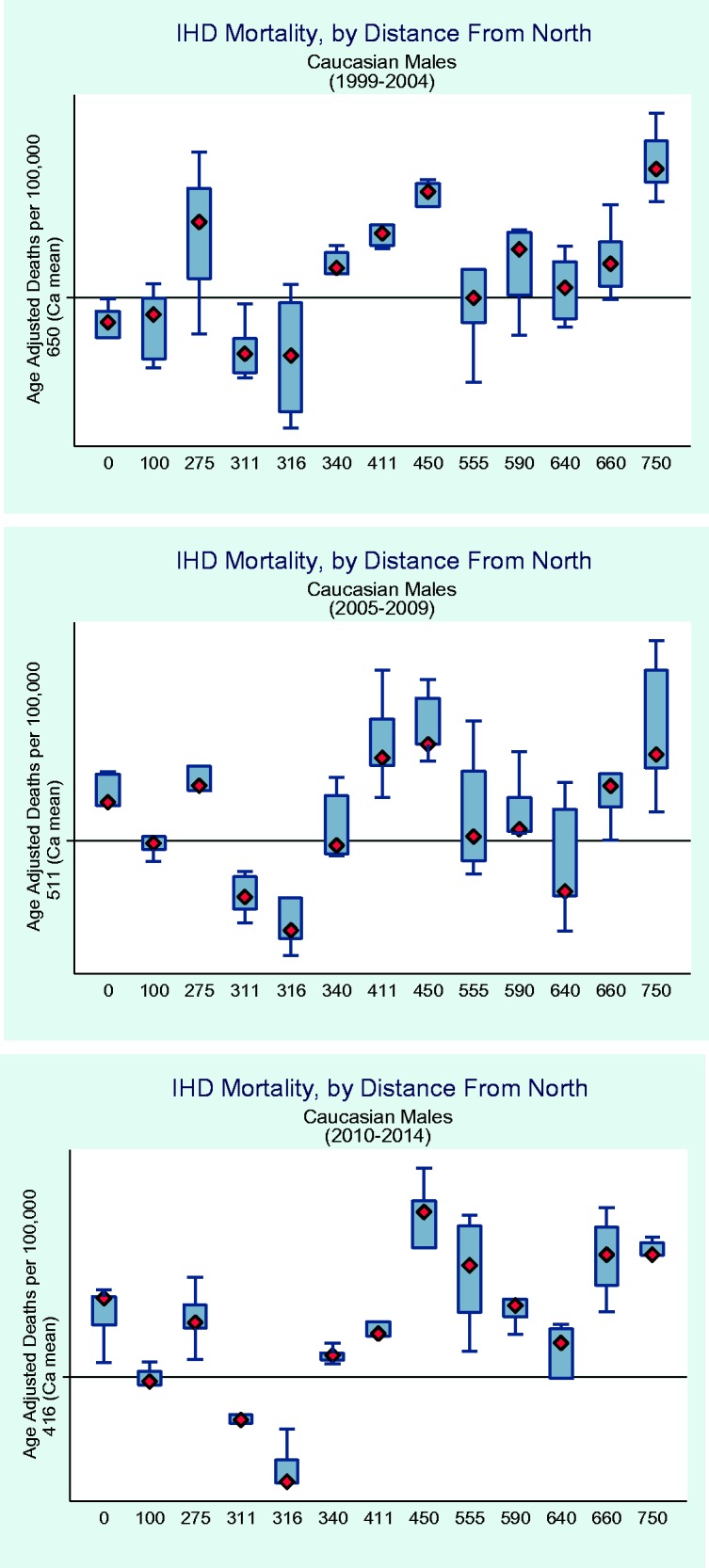
Results: There was an increase in mortality from north to south of 14.9 (95% CI: 8.0-21.9, p value <0.0001) in time period 1, 7.9 (95% CI: 0.8-15, p value <0.05) in time period 2, and 9.2 (95% CI: 4.0-14.3, p value <0.001) in time period 3. In time period 1, the ambient particulate matter ≤2.5 micrometers (PM2.5) level increased from north to south by 0.84 µg/m³ (95% CI: 0.71-0.96), in time period 2 there was a 0.87 µg/m³ increase (95% CI: 0.74-1.0), and a 1.0 µg/m³ increase in time period 3 (95% CI: 0.87-1.1). PM2.5 level was correlated to IHD mortality in all time periods (Period 1 r2 = 0.46, p = 0.0001; Period 2, r2 = 0.34, p = 0.008; Period 3 r2 = 0.51, p value <0.0001).
Conclusion: Continued declines in ischemic heart disease mortality will depend on the concerted efforts of clinicians in continuing management of the traditional risk factors with appropriate medication use, acute interventions for coronary syndromes, the necessity of patient self-management of high risk behaviors associated with smoking and obesity, and the development of coordinated actions with policy makers to reduce environmental exposure in their respective communities.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
