Isabel Tarrio, Marta Moreira, Tarcísio Araújo, Luís Lopes
{"title":"EUS-Guided Choledochoduodenostomy after Failed Endoscopic Retrograde Cholangiopancreatography in Distal Malignant Biliary Obstruction.","authors":"Isabel Tarrio, Marta Moreira, Tarcísio Araújo, Luís Lopes","doi":"10.1159/000528808","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Malignant biliary obstruction drainage is essential, since jaundice is associated with morbidity and mortality. Endoscopic retrograde cholangiopancreatography (ERCP) is the recommended procedure for biliary drainage, with percutaneous biliary drainage being the classic alternative in cases of unsuccessful ERCP. Recently, endoscopic ultrasound-guided biliary drainage has been emerged as a new option, with EUS-guided choledochoduodenostomy (EUS-CDS) being considered an effective and safe method in the drainage of distal obstructions of the common bile duct.</p><p><strong>Aim: </strong>The aim of the study was to evaluate the efficacy and safety of EUS-CDS performed in patients with distal malignant biliary obstructions, after failed ERCP.</p><p><strong>Methods: </strong>Single-center retrospective cohort study between July 2017 and June 2022 including all consecutive patients submitted to EUS-CDS in our center. The primary outcomes were \"technical success\" and \"clinical success,\" defined as \"resolution of jaundice or improvement in total serum bilirubin level above 50% at 7th day and above 75% at 30th day after the procedure.\" Secondary outcomes were procedure-related adverse events, endoscopic reintervention, and survival time.</p><p><strong>Results: </strong>EUS-CDS was performed in 20 patients (65.0% male; median age 76 years). The most frequent etiology for the biliary obstruction was pancreatic adenocarcinoma (<i>n</i> = 17; 85.0%), and most patients presented at advanced stages of cancer (12/60% in stages III or IV). ERCP failure was mainly due to the presence of obstruction in the duodenal lumen (<i>n</i> = 11; 55.0%). Fully covered metallic stents were used in all patients, mostly HotAxios<sup>TM</sup> (<i>n</i> = 15; 75.0%). The technical success rate was 100%, and the clinical success rate was 89.5% (<i>n</i> = 17/19) at 7th day and 93.3% (<i>n</i> = 14/15) at 30th day. Four patients (20.0%) developed cholangitis within the first 30 days after the procedure; there were no late complications, and no patient died as a complication of the procedure. In 2 patients (10.0%), endoscopic reintervention was necessary due to stent migration, incidentally detected. Median survival was 93 days (minimum 5-maximum 751).</p><p><strong>Conclusion: </strong>EUS-CDS was effective in biliary decompression of malignant obstructions of the common bile duct, with high clinical success and a favorable safety profile.</p>","PeriodicalId":51838,"journal":{"name":"GE Portuguese Journal of Gastroenterology","volume":"30 Suppl 1","pages":"65-73"},"PeriodicalIF":0.6000,"publicationDate":"2023-03-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/19/9f/pjg-0030-0065.PMC10561318.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"GE Portuguese Journal of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000528808","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Introduction: Malignant biliary obstruction drainage is essential, since jaundice is associated with morbidity and mortality. Endoscopic retrograde cholangiopancreatography (ERCP) is the recommended procedure for biliary drainage, with percutaneous biliary drainage being the classic alternative in cases of unsuccessful ERCP. Recently, endoscopic ultrasound-guided biliary drainage has been emerged as a new option, with EUS-guided choledochoduodenostomy (EUS-CDS) being considered an effective and safe method in the drainage of distal obstructions of the common bile duct.
Aim: The aim of the study was to evaluate the efficacy and safety of EUS-CDS performed in patients with distal malignant biliary obstructions, after failed ERCP.
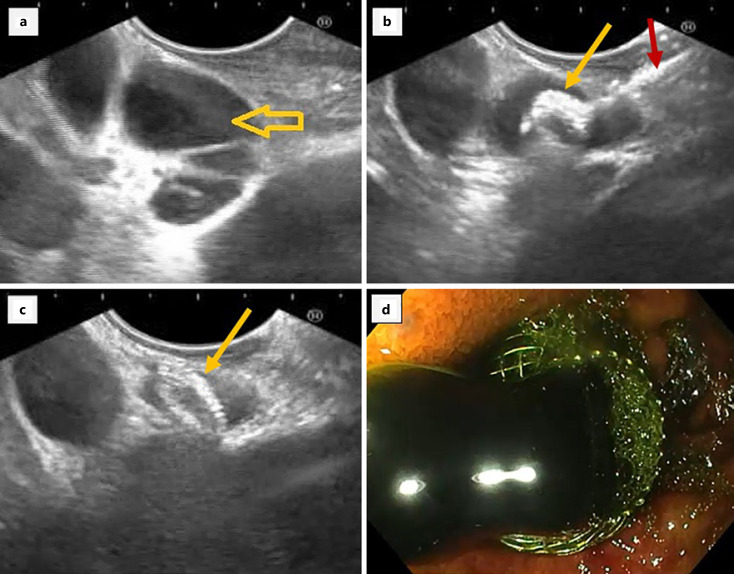
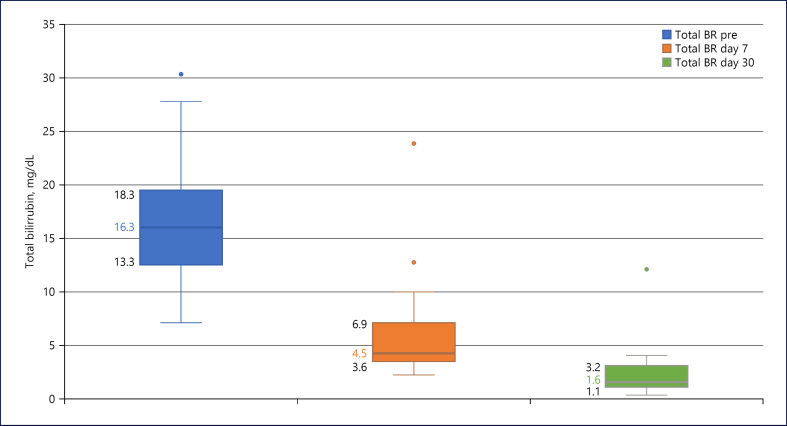
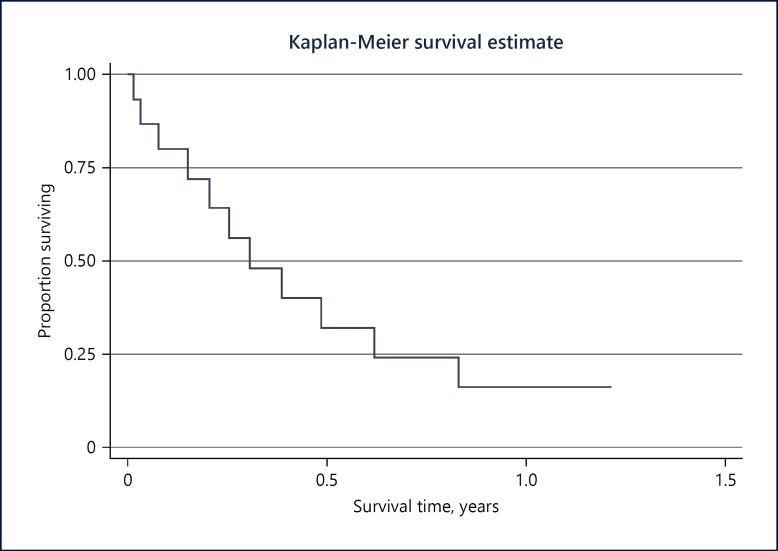
Methods: Single-center retrospective cohort study between July 2017 and June 2022 including all consecutive patients submitted to EUS-CDS in our center. The primary outcomes were "technical success" and "clinical success," defined as "resolution of jaundice or improvement in total serum bilirubin level above 50% at 7th day and above 75% at 30th day after the procedure." Secondary outcomes were procedure-related adverse events, endoscopic reintervention, and survival time.
Results: EUS-CDS was performed in 20 patients (65.0% male; median age 76 years). The most frequent etiology for the biliary obstruction was pancreatic adenocarcinoma (n = 17; 85.0%), and most patients presented at advanced stages of cancer (12/60% in stages III or IV). ERCP failure was mainly due to the presence of obstruction in the duodenal lumen (n = 11; 55.0%). Fully covered metallic stents were used in all patients, mostly HotAxiosTM (n = 15; 75.0%). The technical success rate was 100%, and the clinical success rate was 89.5% (n = 17/19) at 7th day and 93.3% (n = 14/15) at 30th day. Four patients (20.0%) developed cholangitis within the first 30 days after the procedure; there were no late complications, and no patient died as a complication of the procedure. In 2 patients (10.0%), endoscopic reintervention was necessary due to stent migration, incidentally detected. Median survival was 93 days (minimum 5-maximum 751).
Conclusion: EUS-CDS was effective in biliary decompression of malignant obstructions of the common bile duct, with high clinical success and a favorable safety profile.
期刊介绍:
The ''GE Portuguese Journal of Gastroenterology'' (formerly Jornal Português de Gastrenterologia), founded in 1994, is the official publication of Sociedade Portuguesa de Gastrenterologia (Portuguese Society of Gastroenterology), Sociedade Portuguesa de Endoscopia Digestiva (Portuguese Society of Digestive Endoscopy) and Associação Portuguesa para o Estudo do Fígado (Portuguese Association for the Study of the Liver). The journal publishes clinical and basic research articles on Gastroenterology, Digestive Endoscopy, Hepatology and related topics. Review articles, clinical case studies, images, letters to the editor and other articles such as recommendations or papers on gastroenterology clinical practice are also considered. Only articles written in English are accepted.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
