{"title":"Beyond CHNAS: Performance Measurement for Community Health Improvement.","authors":"Michael A Stoto, Mary V Davis, Abby Atkins","doi":"10.5334/egems.312","DOIUrl":null,"url":null,"abstract":"<p><strong>Research objective: </strong>Non-profit hospitals are required to work with community organizations to prepare Community Health Needs Assessment (CHNA) and implementation strategy (IS). In concert with the health care delivery system's transformation from volume to value and efforts to enhance multi-sector collaboration, such community health improvement (CHI) processes have the potential to bridge efforts of the health care delivery sector, public health agencies, and community organizations to improve population health. Having a shared measurement system is critical to achieving collective impact, yet despite the availability of community-level data from a variety of sources, many CHI processes lack clear, measurable objectives and evaluation plans. Through an in-depth analysis of ten exemplary CHI processes, we sought to identify best practices for population health measurement with a focus on monitoring collaborative implementation strategies.</p><p><strong>Study design: </strong>Based on a review of the scientific literature, professional publications and presentations, and nominations from a national advisory panel, we identified 10 exemplary CHI processes. Criteria of choice were whether (1) the CHIs articulate a clear definition of intended outcomes; (2) clear, focused, measurable objectives and expected outcomes, including health equity; (3) expected outcomes are realistic and addressed with specific action plans; and (4) whether the plans and their associated performance measures become fully integrated into agencies and become a way of being for the agencies. We then conducted an in-depth analysis of CHNA, IS, and related documents created by health departments and leading hospitals in each process.</p><p><strong>Population studied: </strong>U.S. hospitals.</p><p><strong>Principal findings: </strong>Community health improvement processes benefit from a shared measurement system that indicate accountability for specific activities. Despite the importance of measurement and evaluation, existing community health improvement efforts often fall short in these areas. There is more variability in format and content of ISs than CHNAs; the most developed models include population-level goals/objectives and strategies with clear accountability and metrics. Other hospital IS's are less developed.Although all U.S. hospitals are familiar with performance measurement in their management, this familiarity does not seem to carry over to Community Benefit and CHNA efforts. Indeed, 5 of the 10 CHI processes we examined have some Accountable Care Organization (ACO) involvement, where population-health performance measures are commonplace. Yet this involvement is not mentioned in the CHNAs and ISs, nor are ACO data cited.</p><p><strong>Conclusions: </strong>Strengthening the CHNA regulations to require that hospitals report the evaluation measures they intend to monitor based on an established community health improvement model could help communities demonstrate impact. As in other areas of health care, performance measures should be tailored to implementation strategy, with clear indication of accountability, and move from outputs to process and outcome measures with established validity and reliability.</p><p><strong>Implications for policy or practice: </strong>Although performance measurement is now commonplace throughout the health care system, the individuals who manage CHI processes may not be that familiar with this approach. This suggests that it is important to develop practitioners' knowledge and skills needed to use it population health data effectively.</p>","PeriodicalId":72880,"journal":{"name":"EGEMS (Washington, DC)","volume":"7 1","pages":"45"},"PeriodicalIF":0.0000,"publicationDate":"2019-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6706995/pdf/","citationCount":"11","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EGEMS (Washington, DC)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5334/egems.312","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 11
Abstract
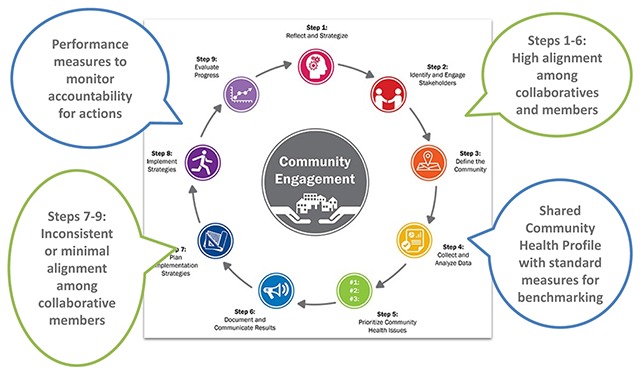
Research objective: Non-profit hospitals are required to work with community organizations to prepare Community Health Needs Assessment (CHNA) and implementation strategy (IS). In concert with the health care delivery system's transformation from volume to value and efforts to enhance multi-sector collaboration, such community health improvement (CHI) processes have the potential to bridge efforts of the health care delivery sector, public health agencies, and community organizations to improve population health. Having a shared measurement system is critical to achieving collective impact, yet despite the availability of community-level data from a variety of sources, many CHI processes lack clear, measurable objectives and evaluation plans. Through an in-depth analysis of ten exemplary CHI processes, we sought to identify best practices for population health measurement with a focus on monitoring collaborative implementation strategies.
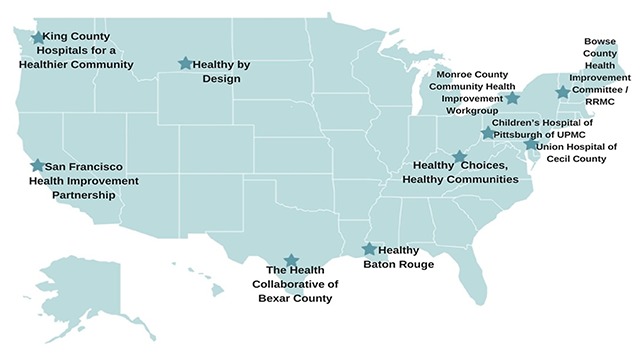
Study design: Based on a review of the scientific literature, professional publications and presentations, and nominations from a national advisory panel, we identified 10 exemplary CHI processes. Criteria of choice were whether (1) the CHIs articulate a clear definition of intended outcomes; (2) clear, focused, measurable objectives and expected outcomes, including health equity; (3) expected outcomes are realistic and addressed with specific action plans; and (4) whether the plans and their associated performance measures become fully integrated into agencies and become a way of being for the agencies. We then conducted an in-depth analysis of CHNA, IS, and related documents created by health departments and leading hospitals in each process.
Population studied: U.S. hospitals.
Principal findings: Community health improvement processes benefit from a shared measurement system that indicate accountability for specific activities. Despite the importance of measurement and evaluation, existing community health improvement efforts often fall short in these areas. There is more variability in format and content of ISs than CHNAs; the most developed models include population-level goals/objectives and strategies with clear accountability and metrics. Other hospital IS's are less developed.Although all U.S. hospitals are familiar with performance measurement in their management, this familiarity does not seem to carry over to Community Benefit and CHNA efforts. Indeed, 5 of the 10 CHI processes we examined have some Accountable Care Organization (ACO) involvement, where population-health performance measures are commonplace. Yet this involvement is not mentioned in the CHNAs and ISs, nor are ACO data cited.
Conclusions: Strengthening the CHNA regulations to require that hospitals report the evaluation measures they intend to monitor based on an established community health improvement model could help communities demonstrate impact. As in other areas of health care, performance measures should be tailored to implementation strategy, with clear indication of accountability, and move from outputs to process and outcome measures with established validity and reliability.
Implications for policy or practice: Although performance measurement is now commonplace throughout the health care system, the individuals who manage CHI processes may not be that familiar with this approach. This suggests that it is important to develop practitioners' knowledge and skills needed to use it population health data effectively.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
