Diana Jo, Nisha Gupta, David Bastawrous, Hayley Busch, Asha Neptune, Amy Weis, Courtney Port
{"title":"Reducing Overutilization of High-flow Nasal Cannula in Children with Bronchiolitis.","authors":"Diana Jo, Nisha Gupta, David Bastawrous, Hayley Busch, Asha Neptune, Amy Weis, Courtney Port","doi":"10.1097/pq9.0000000000000690","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Bronchiolitis is a leading cause of pediatric hospitalizations. A high-flow nasal cannula (HFNC) does not significantly improve clinical outcomes and is associated with increased costs and intensive care unit (ICU) utilization. Despite this, hospitals continue to overuse HFNC in children with bronchiolitis. We aimed to reduce HFNC initiation in children hospitalized with bronchiolitis by 20 percentage points within 6 months.</p><p><strong>Methods: </strong>This study included patients aged 1 month to 2 years diagnosed with bronchiolitis, excluding patients with prematurity less than 32 weeks or preexisting cardiopulmonary, genetic, congenital, or neuromuscular abnormalities. Measures included HFNC utilization, length of stay, length of oxygen supplementation (LOOS), ICU transfers, and emergency department (ED) revisits and readmissions. For our primary intervention, we implemented a HFNC initiation protocol incorporating a respiratory scoring system, a multidisciplinary care-team huddle, and an emphasis on supportive care. Staff education, electronic health record integration, and audit and feedback were used to support implementation. Statistical process control charts were used to track metrics.</p><p><strong>Results: </strong>We analyzed 325 hospitalizations (126 baseline and 199 postintervention). The proportion of children hospitalized with bronchiolitis who received HFNC decreased from a mean of 82% to 60% within 1 month of implementation. Length of stay decreased from a median of 54 to 42 hours, and length of oxygen supplementation decreased from 50 to 38 hours. There were no significant changes in ICU transfers, 7-day ED revisits, or readmissions.</p><p><strong>Conclusions: </strong>Implementing a HFNC initiation protocol can safely reduce the overutilization of HFNC in children hospitalized with bronchiolitis.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"8 5","pages":"e690"},"PeriodicalIF":1.1000,"publicationDate":"2023-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10561806/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000690","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Bronchiolitis is a leading cause of pediatric hospitalizations. A high-flow nasal cannula (HFNC) does not significantly improve clinical outcomes and is associated with increased costs and intensive care unit (ICU) utilization. Despite this, hospitals continue to overuse HFNC in children with bronchiolitis. We aimed to reduce HFNC initiation in children hospitalized with bronchiolitis by 20 percentage points within 6 months.
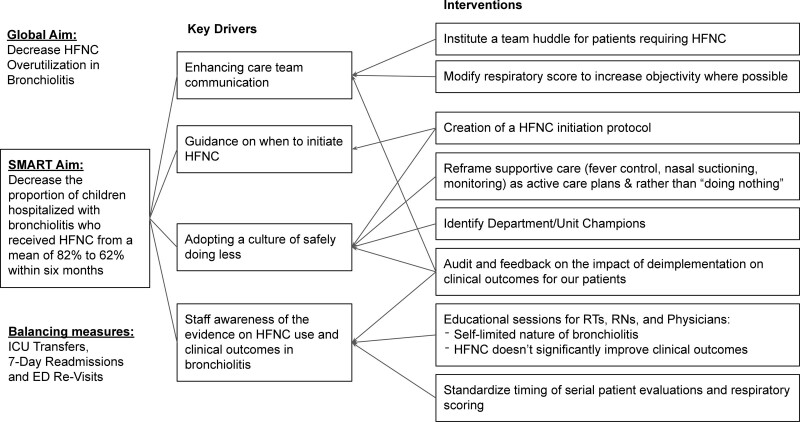
Methods: This study included patients aged 1 month to 2 years diagnosed with bronchiolitis, excluding patients with prematurity less than 32 weeks or preexisting cardiopulmonary, genetic, congenital, or neuromuscular abnormalities. Measures included HFNC utilization, length of stay, length of oxygen supplementation (LOOS), ICU transfers, and emergency department (ED) revisits and readmissions. For our primary intervention, we implemented a HFNC initiation protocol incorporating a respiratory scoring system, a multidisciplinary care-team huddle, and an emphasis on supportive care. Staff education, electronic health record integration, and audit and feedback were used to support implementation. Statistical process control charts were used to track metrics.
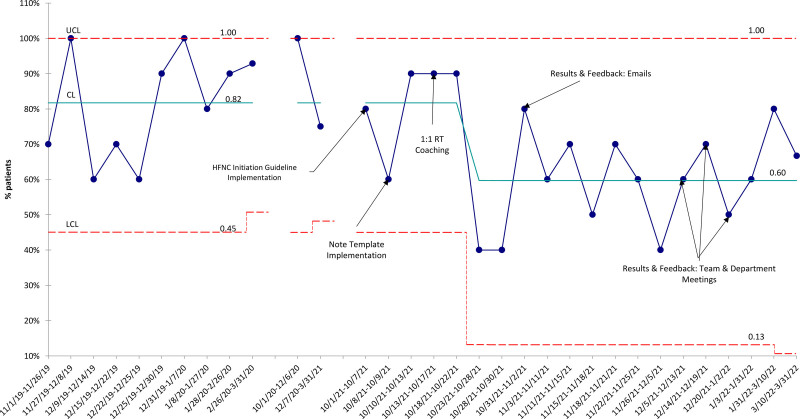
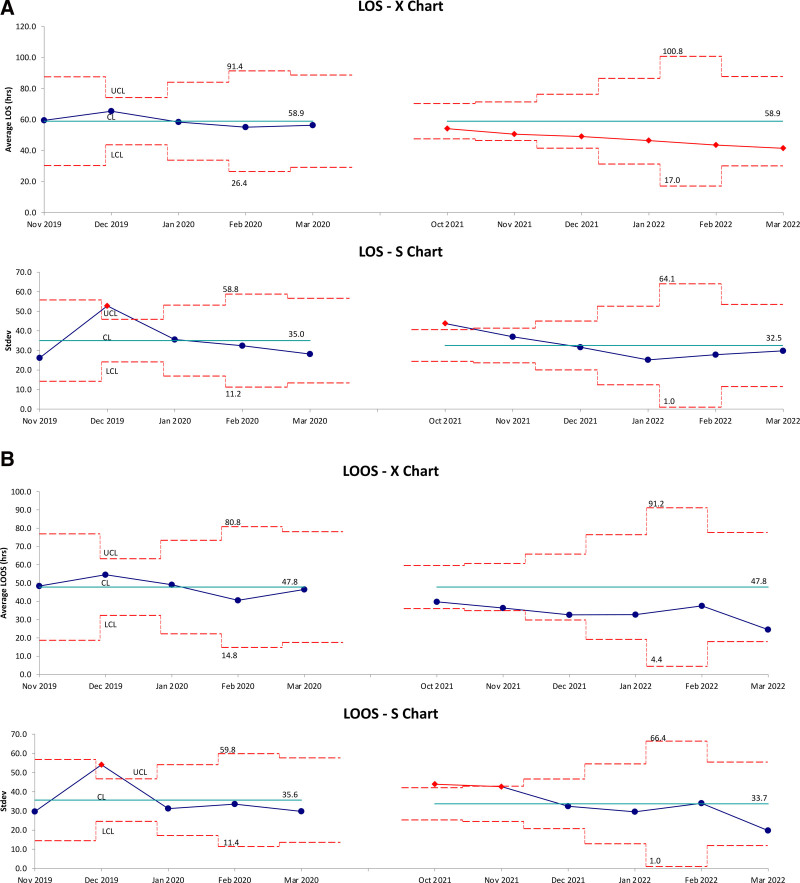
Results: We analyzed 325 hospitalizations (126 baseline and 199 postintervention). The proportion of children hospitalized with bronchiolitis who received HFNC decreased from a mean of 82% to 60% within 1 month of implementation. Length of stay decreased from a median of 54 to 42 hours, and length of oxygen supplementation decreased from 50 to 38 hours. There were no significant changes in ICU transfers, 7-day ED revisits, or readmissions.
Conclusions: Implementing a HFNC initiation protocol can safely reduce the overutilization of HFNC in children hospitalized with bronchiolitis.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
