Salvage of failed direct lateral sacroiliac joint fixation using a new percutaneous lateral-oblique transfixation technique with two variable-threaded screws: a multicenter case report of three cases.
Kingsley R Chin, Richard R Francis, William M Costigan, Erik Spayde, Chidubem Ike, Yujin Jeong, Deepak K Pandey, Jason A Seale
{"title":"Salvage of failed direct lateral sacroiliac joint fixation using a new percutaneous lateral-oblique transfixation technique with two variable-threaded screws: a multicenter case report of three cases.","authors":"Kingsley R Chin, Richard R Francis, William M Costigan, Erik Spayde, Chidubem Ike, Yujin Jeong, Deepak K Pandey, Jason A Seale","doi":"10.21037/jss-23-43","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The direct lateral trans-gluteal muscle splitting transiliac approach was popularized to fixate the sacroiliac joint (SIJ) using three cannulated triangular titanium implants (TTIs) wedges. Publications support efficacy of the direct lateral approach but a paucity of literature to help surgeons revise these implants when they fail. Intuitively the implants can be removed but require an open incision and dissection through the gluteal muscles and scar tissue which can lead to muscle and neurovascular injuries. Our objective was to evaluate the clinical outcome, measured by patient-reported Visual Analog Score (VAS), of three patients who had failed direct lateral SIJ fusions each using three implants and describe a revision technique using a new percutaneous lateral-oblique transfixation technique with two variable-threaded screws while preserving the original implants.</p><p><strong>Case description: </strong>Two separate orthopedic spine surgeons at different hospitals performed the technique using two SacroFuse<sup>®</sup> screws for SIJ revision fusion in three patients who had clinical symptoms and radiographic findings of SIJ pseudoarthrosis after direct lateral approach. One 61 years old male patient had a previous surgery with three lateral threaded screw implants. Two females with ages 47 and 40 years old had three TTI wedges. Follow-up from 10 to 26 months. Patients discharged home the same day. Mean procedure time of 20 minutes with blood loss less than five cc. Incision size was approximately 1 inch. Each patient had a 12 mm × 60 mm and a 12 mm × 50 mm screw filled with NanoFuse Biologics synthetic bioactive glass and demineralized bone matrix. Prior implants were left in place. There was an 89% decrease in mean VAS score of 9.5 to 1.</p><p><strong>Conclusions: </strong>This is a clinically valuable report because until now there was no reconstructive surgery to revise direct lateral implants other than removal with potential neurovascular risks. This is the first article to demonstrate a lateral-oblique transfixation technique with two variable-threaded screws for successful salvage of SIJ pseudoarthrosis after direct lateral fixation without implant removal. The Sacrix technique achieved immediate stability and long-term fusion documented on computed tomography (CT) scan as early as 6 months.</p>","PeriodicalId":17131,"journal":{"name":"Journal of spine surgery","volume":"9 3","pages":"348-356"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/74/29/jss-09-03-348.PMC10570639.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of spine surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/jss-23-43","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The direct lateral trans-gluteal muscle splitting transiliac approach was popularized to fixate the sacroiliac joint (SIJ) using three cannulated triangular titanium implants (TTIs) wedges. Publications support efficacy of the direct lateral approach but a paucity of literature to help surgeons revise these implants when they fail. Intuitively the implants can be removed but require an open incision and dissection through the gluteal muscles and scar tissue which can lead to muscle and neurovascular injuries. Our objective was to evaluate the clinical outcome, measured by patient-reported Visual Analog Score (VAS), of three patients who had failed direct lateral SIJ fusions each using three implants and describe a revision technique using a new percutaneous lateral-oblique transfixation technique with two variable-threaded screws while preserving the original implants.
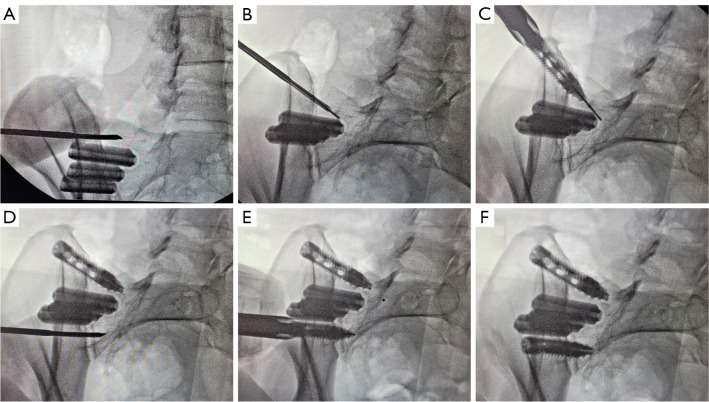
Case description: Two separate orthopedic spine surgeons at different hospitals performed the technique using two SacroFuse® screws for SIJ revision fusion in three patients who had clinical symptoms and radiographic findings of SIJ pseudoarthrosis after direct lateral approach. One 61 years old male patient had a previous surgery with three lateral threaded screw implants. Two females with ages 47 and 40 years old had three TTI wedges. Follow-up from 10 to 26 months. Patients discharged home the same day. Mean procedure time of 20 minutes with blood loss less than five cc. Incision size was approximately 1 inch. Each patient had a 12 mm × 60 mm and a 12 mm × 50 mm screw filled with NanoFuse Biologics synthetic bioactive glass and demineralized bone matrix. Prior implants were left in place. There was an 89% decrease in mean VAS score of 9.5 to 1.
Conclusions: This is a clinically valuable report because until now there was no reconstructive surgery to revise direct lateral implants other than removal with potential neurovascular risks. This is the first article to demonstrate a lateral-oblique transfixation technique with two variable-threaded screws for successful salvage of SIJ pseudoarthrosis after direct lateral fixation without implant removal. The Sacrix technique achieved immediate stability and long-term fusion documented on computed tomography (CT) scan as early as 6 months.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
