{"title":"Cervical Fracture with Diffuse Idiopathic Skeletal Hyperostosis and Respiratory Insufficiency: A Case Report.","authors":"Kengo Fujii, Toru Funayama, Kaishi Ogawa, Sayori Li, Masashi Yamazaki","doi":"10.22603/ssrr.2022-0231","DOIUrl":null,"url":null,"abstract":"Diffuse idiopathic skeletal hyperostosis (DISH) reportedly increases the risk of fracture due to low-energy trauma. Countries with an increasing aging population have an increased incidence of cervical trauma in elderly patients, mostly occurring in the setting of low-energy trauma. We report a rare case of cervical fracture with DISH and subsequent respiratory insufficiency managed by emergency anterior cervical surgery. An 87-year-old man was brought in by an ambulance and transferred to our hospital 4 h after a fall on the floor. He lost consciousness for 2 h following the fall and woke up with muscle weakness. His past medical and surgical histories included hypertension, atrial arrhythmia, and cerebellar infarction with residual mild paralysis in his right upper and lower limbs. The patient was taking oral rivaroxaban. Plain radiography and computed tomography (CT) revealed ossification of the posterior longitudinal ligament at C3-5, fusion due to the ossification of the anterior longitudinal ligament (OALL) at C5-7, fusion due to DISH at C5-7 and T2-12 (Fig. 1), and a fracture involving the OALL at the C6/7 intervertebral disc level. Magnetic resonance imaging (MRI) slices showed a large retropharyngeal hematoma extending to the mediastinum. Moreover, cervical spinal canal stenosis and myelomalacia at the C3/4 and C4/5 levels were observed, which showed the spinal cord injury (Fig. 2). At that point, muscle strength was fully recovered, although he reported severe paresthesia in both hands. Dyspnea and respiratory insufficiency occurred 6 h after the presentation. Tracheal intubation was performed, and the patient was ventilated. Arterial active bleeding was still observed after 10 coiling attempts by transcatheter angiography (Fig. 3). Therefore, we decided to perform emergency anterior cervical surgery (Fig. 4). A large hematoma extending from the retropharyngeal re-","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"7 5","pages":"468-472"},"PeriodicalIF":1.2000,"publicationDate":"2023-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ef/6a/2432-261X-7-0468.PMC10569800.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2022-0231","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/27 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
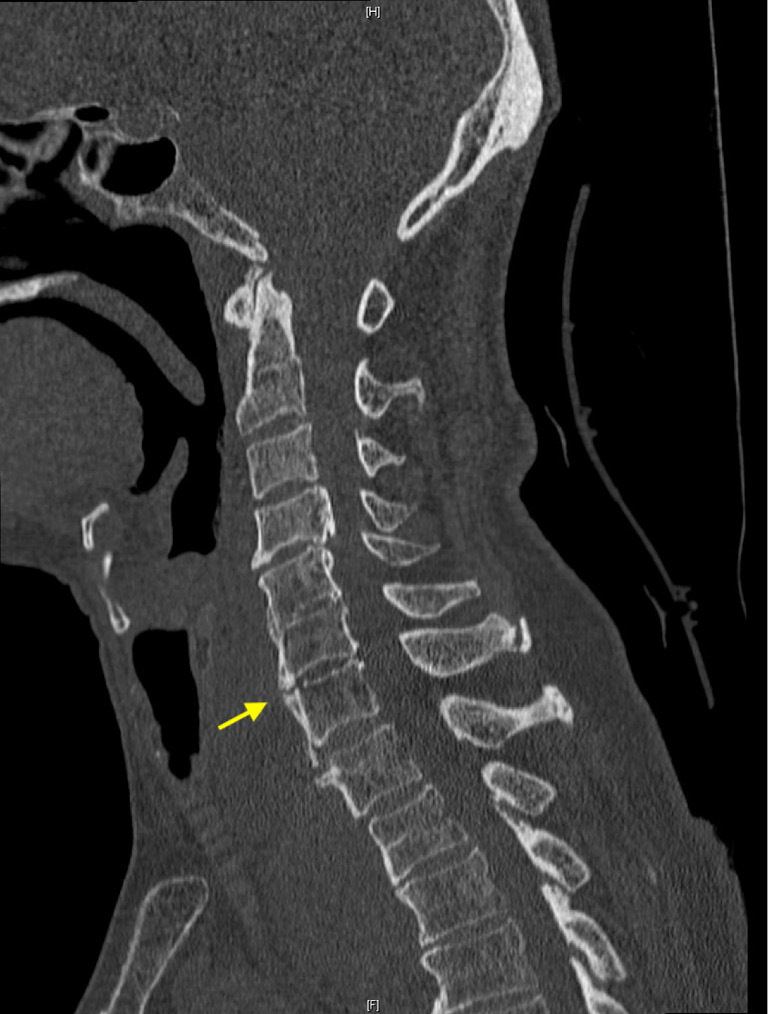
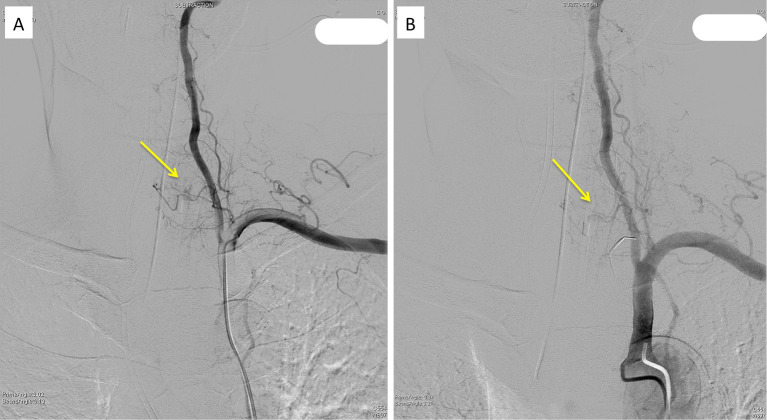
Diffuse idiopathic skeletal hyperostosis (DISH) reportedly increases the risk of fracture due to low-energy trauma. Countries with an increasing aging population have an increased incidence of cervical trauma in elderly patients, mostly occurring in the setting of low-energy trauma. We report a rare case of cervical fracture with DISH and subsequent respiratory insufficiency managed by emergency anterior cervical surgery. An 87-year-old man was brought in by an ambulance and transferred to our hospital 4 h after a fall on the floor. He lost consciousness for 2 h following the fall and woke up with muscle weakness. His past medical and surgical histories included hypertension, atrial arrhythmia, and cerebellar infarction with residual mild paralysis in his right upper and lower limbs. The patient was taking oral rivaroxaban. Plain radiography and computed tomography (CT) revealed ossification of the posterior longitudinal ligament at C3-5, fusion due to the ossification of the anterior longitudinal ligament (OALL) at C5-7, fusion due to DISH at C5-7 and T2-12 (Fig. 1), and a fracture involving the OALL at the C6/7 intervertebral disc level. Magnetic resonance imaging (MRI) slices showed a large retropharyngeal hematoma extending to the mediastinum. Moreover, cervical spinal canal stenosis and myelomalacia at the C3/4 and C4/5 levels were observed, which showed the spinal cord injury (Fig. 2). At that point, muscle strength was fully recovered, although he reported severe paresthesia in both hands. Dyspnea and respiratory insufficiency occurred 6 h after the presentation. Tracheal intubation was performed, and the patient was ventilated. Arterial active bleeding was still observed after 10 coiling attempts by transcatheter angiography (Fig. 3). Therefore, we decided to perform emergency anterior cervical surgery (Fig. 4). A large hematoma extending from the retropharyngeal re-




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
