{"title":"Deep Segmentation Feature-Based Radiomics Improves Recurrence Prediction of Hepatocellular Carcinoma.","authors":"Jifei Wang, Dasheng Wu, Meili Sun, Zhenpeng Peng, Yingyu Lin, Hongxin Lin, Jiazhao Chen, Tingyu Long, Zi-Ping Li, Chuanmiao Xie, Bingsheng Huang, Shi-Ting Feng","doi":"10.34133/2022/9793716","DOIUrl":null,"url":null,"abstract":"<p><p><i>Objective and Impact Statement</i>. This study developed and validated a deep semantic segmentation feature-based radiomics (DSFR) model based on preoperative contrast-enhanced computed tomography (CECT) combined with clinical information to predict early recurrence (ER) of single hepatocellular carcinoma (HCC) after curative resection. ER prediction is of great significance to the therapeutic decision-making and surveillance strategy of HCC. <i>Introduction</i>. ER prediction is important for HCC. However, it cannot currently be adequately determined. <i>Methods</i>. Totally, 208 patients with single HCC after curative resection were retrospectively recruited into a model-development cohort (<math><mi>n</mi><mo>=</mo><mn>180</mn></math>) and an independent validation cohort (<math><mi>n</mi><mo>=</mo><mn>28</mn></math>). DSFR models based on different CT phases were developed. The optimal DSFR model was incorporated with clinical information to establish a DSFR-C model. An integrated nomogram based on the Cox regression was established. The DSFR signature was used to stratify high- and low-risk ER groups. <i>Results</i>. A portal phase-based DSFR model was selected as the optimal model (area under receiver operating characteristic curve (AUC): development cohort, 0.740; validation cohort, 0.717). The DSFR-C model achieved AUCs of 0.782 and 0.744 in the development and validation cohorts, respectively. In the development and validation cohorts, the integrated nomogram achieved C-index of 0.748 and 0.741 and time-dependent AUCs of 0.823 and 0.822, respectively, for recurrence-free survival (RFS) prediction. The RFS difference between the risk groups was statistically significant (<math><mi>P</mi><mo><</mo><mn>0.0001</mn></math> and <math><mi>P</mi><mo>=</mo><mn>0.045</mn></math> in the development and validation cohorts, respectively). <i>Conclusion</i>. CECT-based DSFR can predict ER in single HCC after curative resection, and its combination with clinical information further improved the performance for ER prediction.</p>","PeriodicalId":72430,"journal":{"name":"BME frontiers","volume":"2022 ","pages":"9793716"},"PeriodicalIF":7.7000,"publicationDate":"2022-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10521680/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BME frontiers","FirstCategoryId":"1087","ListUrlMain":"https://doi.org/10.34133/2022/9793716","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
引用次数: 2
Abstract
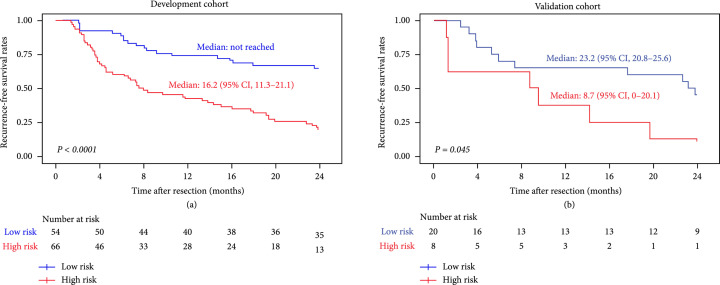
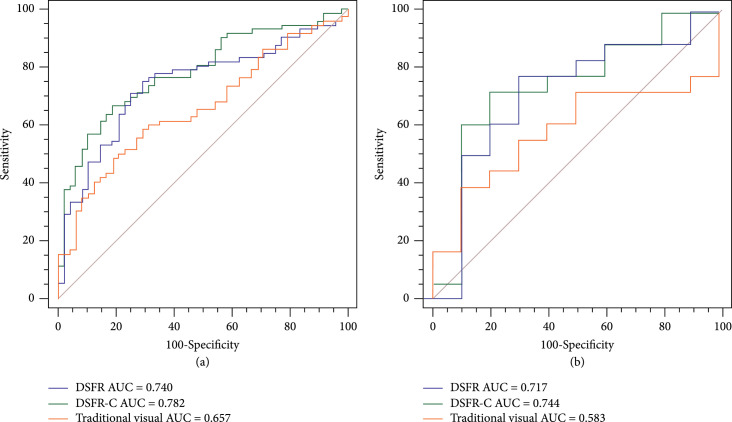
Objective and Impact Statement. This study developed and validated a deep semantic segmentation feature-based radiomics (DSFR) model based on preoperative contrast-enhanced computed tomography (CECT) combined with clinical information to predict early recurrence (ER) of single hepatocellular carcinoma (HCC) after curative resection. ER prediction is of great significance to the therapeutic decision-making and surveillance strategy of HCC. Introduction. ER prediction is important for HCC. However, it cannot currently be adequately determined. Methods. Totally, 208 patients with single HCC after curative resection were retrospectively recruited into a model-development cohort () and an independent validation cohort (). DSFR models based on different CT phases were developed. The optimal DSFR model was incorporated with clinical information to establish a DSFR-C model. An integrated nomogram based on the Cox regression was established. The DSFR signature was used to stratify high- and low-risk ER groups. Results. A portal phase-based DSFR model was selected as the optimal model (area under receiver operating characteristic curve (AUC): development cohort, 0.740; validation cohort, 0.717). The DSFR-C model achieved AUCs of 0.782 and 0.744 in the development and validation cohorts, respectively. In the development and validation cohorts, the integrated nomogram achieved C-index of 0.748 and 0.741 and time-dependent AUCs of 0.823 and 0.822, respectively, for recurrence-free survival (RFS) prediction. The RFS difference between the risk groups was statistically significant ( and in the development and validation cohorts, respectively). Conclusion. CECT-based DSFR can predict ER in single HCC after curative resection, and its combination with clinical information further improved the performance for ER prediction.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
