{"title":"Early periprosthetic hip joint infection managed by cementless one-stage revision - a case series.","authors":"Kristoffer Riemer, Jeppe Lange","doi":"10.5194/jbji-7-43-2022","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b>: Early periprosthetic hip joint infection (PJI) is traditionally treated with debridement, antibiotics, and implant retention (DAIR). However, infection control rates after DAIR-treated periprosthetic hip joint infection do not exceed 77 %. Cementless one-stage revision of chronic PJI by the Cementless One-stage Revision of Infected Hip Arthroplasty (CORIHA) protocol has been evaluated positively with a 91 % success rate. We wanted to evaluate the effectiveness of cementless one-stage revision following the CORIHA protocol for early PJI in elective primary total hip arthroplasty, regarding risk of re-operation with exchange of implants. <b>Methods</b>: We identified 18 patients in our center with early ( <math><mrow><mo>≤</mo> <mn>6</mn></mrow> </math> -week postoperative) PJI after primary total hip arthroplasty (THA) treated with one-stage cementless revision in the period January 2012-March 2018. Treatment followed the CORIHA protocol. Primary outcome was retention of implants at the most recent follow-up. Patients were followed for a minimum of 3 years. <b>Results</b>: Mean follow-up time was 60 months (39-105). All patients retained their implants, but two required superficial soft tissue debridement due to persistent wound seepage. <b>Conclusion</b>: Cementless one-stage revision appears to be an effective treatment of early PJI after primary THA and at least an equal choice of treatment compared with DAIR. Whether the potential benefit of a lower re-revision rate for postoperative PJI outweighs the increased surgical complexity of the CORIHA procedure needs further evaluation.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":"7 1","pages":"43-50"},"PeriodicalIF":2.8000,"publicationDate":"2022-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8892566/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-7-43-2022","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
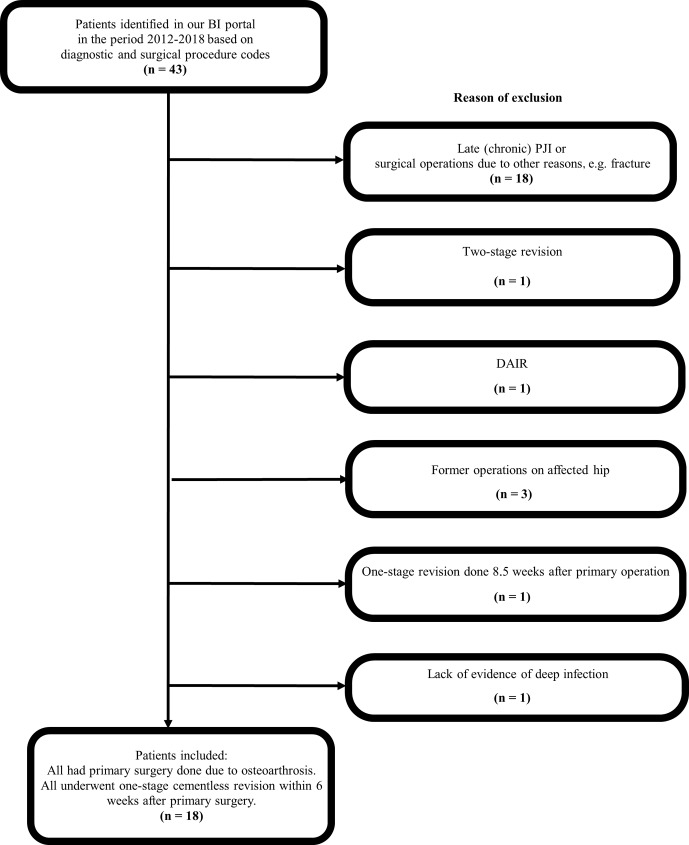
Background: Early periprosthetic hip joint infection (PJI) is traditionally treated with debridement, antibiotics, and implant retention (DAIR). However, infection control rates after DAIR-treated periprosthetic hip joint infection do not exceed 77 %. Cementless one-stage revision of chronic PJI by the Cementless One-stage Revision of Infected Hip Arthroplasty (CORIHA) protocol has been evaluated positively with a 91 % success rate. We wanted to evaluate the effectiveness of cementless one-stage revision following the CORIHA protocol for early PJI in elective primary total hip arthroplasty, regarding risk of re-operation with exchange of implants. Methods: We identified 18 patients in our center with early ( -week postoperative) PJI after primary total hip arthroplasty (THA) treated with one-stage cementless revision in the period January 2012-March 2018. Treatment followed the CORIHA protocol. Primary outcome was retention of implants at the most recent follow-up. Patients were followed for a minimum of 3 years. Results: Mean follow-up time was 60 months (39-105). All patients retained their implants, but two required superficial soft tissue debridement due to persistent wound seepage. Conclusion: Cementless one-stage revision appears to be an effective treatment of early PJI after primary THA and at least an equal choice of treatment compared with DAIR. Whether the potential benefit of a lower re-revision rate for postoperative PJI outweighs the increased surgical complexity of the CORIHA procedure needs further evaluation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
