Dicky L. Tahapary, Syahidatul Wafa, Christian Tricaesario, Felix F. Widjaja, Jimmy Tandradynata, Rudy Kurniawan, William Djauhari, Afif H. Maruf, Muhammad Yamin, Sidartawan Soegondo
{"title":"Chronic complications risk among type 2 diabetes patients with a family history of diabetes","authors":"Dicky L. Tahapary, Syahidatul Wafa, Christian Tricaesario, Felix F. Widjaja, Jimmy Tandradynata, Rudy Kurniawan, William Djauhari, Afif H. Maruf, Muhammad Yamin, Sidartawan Soegondo","doi":"10.1002/cdt3.80","DOIUrl":null,"url":null,"abstract":"<p>Family history of diabetes (FH+) has been associated with early metabolic alteration including insulin resistance, lipid metabolism, and ectopic fat accumulation even in healthy individuals.<span><sup>1-3</sup></span> Furthermore, normoglycemic first-degree relatives of type 2 diabetes mellitus (T2DM) have been documented having increased carotid intima-media thickness and pro-inflammatory cytokines.<span><sup>4, 5</sup></span> Taken together, individuals with FH+, who were otherwise healthy, have shown to possess susceptibility for diabetes mellitus (DM) chronic complication. Hence, this study aimed to investigate whether FH+ increased the risk of chronic complications in patients with overt T2DM.</p><p>This was a cross-sectional study which included adult patients with T2DM visiting a private hospital integrated diabetes center in South Tangerang (urban area outskirt of Jakarta), Indonesia from December 2020 to November 2021. Those without any documented blood test results were excluded. FH+ was defined as having first- and/or second-degree relatives with T2DM. Chronic complications investigated were atherosclerotic cardiovascular diseases (ASCVD) including coronary artery disease (CAD), stroke, and peripheral artery disease; microvascular complications including diabetic retinopathy, diabetic peripheral neuropathy, and diabetic kidney disease (DKD); diastolic dysfunction and heart failure (HF). Data were taken from hospital electronic medical records and were explored from clinical signs and symptoms, history of previously known chronic complications, laboratory and radiological examinations, and diagnosis made by the physicians. Additionally, if any, other tests were used for diagnosis such as treadmill stress test and coronary arteries calcium scoring for CAD; ankle-to-brachial index of ≤0.9 and limb vessels stenosis of ≥50% on doppler ultrasound for peripheral artery disease; non-mydriatic funduscopy for retinopathy; 10 g monofilament test and 128 Hz tuning fork test for neuropathy; presence of micro-/macroalbuminuria or proteinuria and glomerular filtration rate ≤60 mL/min for DKD; echocardiography for diastolic dysfunction and HF.</p><p>Results were presented in <i>n</i> (%), and median (interquartile range, IQR) depends on data type. Chi-squared test was used to compare nominal data, while Mann–Whitney was used to compare numerical data. Logistic regression analysis was used to determine FH+ association with chronic complications adjusted for age, sex, DM duration, alcohol and smoking history, systolic and diastolic blood pressure, body mass index, HbA1c, low-density lipoprotein, triglyceride, and estimated glomerular filtration rate, with no family history of diabetes (FH−) as the reference.</p><p>A total of 1011 T2DM patients were included, 24.8% of whom had family history of T2DM (FH+) (Table 1). There were higher proportions of dyslipidemia, smoking and alcohol history found in FH+, whereas FH− had older age, higher systolic blood pressure and triglyceride level, and lower eGFR (Table 1).</p><p>Overall, higher proportions of complications were seen in FH+, but statistical significances were mainly for microvascular complications, not for ASCVD (Figure 1). In multivariate analysis, FH+ remained significantly associated with diastolic dysfunction (adjusted odds ratio [aOR]: 4.16 [2.58–6.69]), retinopathy (aOR: 3.76 [1.94–7.28]), peripheral neuropathy (aOR: 3.20 [2.02–5.05]), composite microvascular complications (aOR: 1.93 [1.26–2.96]), and composite macro- and micro-vascular complications (aOR: 1.83 [1.09–3.08]) (Figure 2).</p><p>In this study, we observed a higher proportion of dyslipidemia and a history of smoking and alcohol in FH+ compared to those in FH− group. Nevertheless, having a family history of diabetes was independently associated with increased risks of developing chronic complications, especially diastolic dysfunction, retinopathy, and peripheral neuropathy.</p><p>Despite some statistically significant differences in baseline characteristics between FH+ and FH− subjects, it was of no clinical significance. Indeed, we noticed that FH+ patients in our study tended to drink alcohol and smoke in comparison to those in FH− groups. This might contribute to a higher prevalence of dyslipidemia<span><sup>6</sup></span> in FH+, in addition to the known increased risk of dyslipidemia possessed by having a family history of diabetes.<span><sup>1, 2</sup></span></p><p>FH+ was independently associated with microvascular complications (retinopathy and neuropathy), but not with any ASCVD. In line with previous studies, FH+ was associated with retinopathy and neuropathy but not with DKD<span><sup>7-10</sup></span>; and that family history of CAD or stroke were stronger predictors for ASCVD than family history of diabetes.<span><sup>10-12</sup></span></p><p>FH+ has been associated with younger onset of diabetes, which was characterized by poor glycemic control and more progressive complications.<span><sup>13, 14</sup></span> Offspring of T2DM has been reported to demonstrate oxidative stress upregulation following high-carbohydrate challenge, in addition to dysregulated antioxidative status, compared to those in the FH- counterpart with similar metabolic profile.<span><sup>15, 16</sup></span></p><p>Previous studies observed that systolic blood pressure was associated with an increased risk of diastolic dysfunction.<span><sup>17, 18</sup></span> Interestingly, in our study, we found that FH+ was independent predictor of diastolic dysfunction despite lower systolic blood pressure compared to those of FH–. Based on our multivariate analysis, it seems that FH+ impact on diastolic dysfunction surpassed that of systolic blood pressure. On further analysis, both groups had similar proportions of patients having systolic blood pressure under 140 mmHg (61.6% vs. 54.2%, <i>p</i> = 0.055) and 130 mmHg (37.9% vs. 32.1%, <i>p</i> = 0.113), implicating that clinically both groups had similar blood pressure control which might also explain our findings. The mechanism by which FH+ was at higher risk of diastolic dysfunction might be due to impaired cardiac endothelial glycocalyx, autonomic function and relaxation performance.<span><sup>16, 19</sup></span></p><p>Prior hyperglycemic exposure was reported to have long-term effect, called “metabolic memory.”<span><sup>20</sup></span> Patients with FH+, who were associated with younger onset age and poor glycemic control,<span><sup>14</sup></span> might be disadvantaged from metabolic memory. Epigenetic mechanisms have been thought of as the contributing factor.<span><sup>20</sup></span></p><p>The unavailability of data regarding age of DM onset and socioeconomic status was one of the limitations of this study. Additionally, retrospective data extraction resulted in some missing examination results. Further research investigating whether FH+ has different epigenetic mechanisms, compared to FH−, as response to similar environmental and metabolic factors is yet to be explored.</p><p>In conclusion, T2DM patients with a family history of diabetes had an increased risk for having diastolic dysfunction and microvascular complications. While in the clinical setting this should imply a more rigorous management for this group of patients, in terms of research, further studies are needed to unravel the underlying mechanism.</p><p>All authors participated in the conceptualization, methodology, and interpretation of study results. Christian Tricaesario conducted the investigation. William Djauhari and Afif H. Maruf organized data curation. Christian Tricaesario, William Djauhari, and Afif H. Maruf wrote the original draft. Christian Tricaesario did the formal analysis and prepared the visualization of the study results. Dicky L. Tahapary critically reviewed the study, advised on analysis, the visualization of study results, data interpretation, and revised the manuscript. Syahidatul Wafa, Felix F. Widjaja, Jimmy Tandradynata, Rudy Kurniawan, and Muhammad Yamin critically reviewed the article. Sidartawan Soegondo supervised, critically reviewed, and validated the study. All authors have approved the final manuscript.</p><p>The authors declare no conflict of interest.</p><p>This study was approved by the Ethics Committee of the Faculty of Medicine Universitas Indonesia.</p>","PeriodicalId":32096,"journal":{"name":"Chronic Diseases and Translational Medicine","volume":"9 4","pages":"336-340"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Diseases and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.80","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Family history of diabetes (FH+) has been associated with early metabolic alteration including insulin resistance, lipid metabolism, and ectopic fat accumulation even in healthy individuals.1-3 Furthermore, normoglycemic first-degree relatives of type 2 diabetes mellitus (T2DM) have been documented having increased carotid intima-media thickness and pro-inflammatory cytokines.4, 5 Taken together, individuals with FH+, who were otherwise healthy, have shown to possess susceptibility for diabetes mellitus (DM) chronic complication. Hence, this study aimed to investigate whether FH+ increased the risk of chronic complications in patients with overt T2DM.
This was a cross-sectional study which included adult patients with T2DM visiting a private hospital integrated diabetes center in South Tangerang (urban area outskirt of Jakarta), Indonesia from December 2020 to November 2021. Those without any documented blood test results were excluded. FH+ was defined as having first- and/or second-degree relatives with T2DM. Chronic complications investigated were atherosclerotic cardiovascular diseases (ASCVD) including coronary artery disease (CAD), stroke, and peripheral artery disease; microvascular complications including diabetic retinopathy, diabetic peripheral neuropathy, and diabetic kidney disease (DKD); diastolic dysfunction and heart failure (HF). Data were taken from hospital electronic medical records and were explored from clinical signs and symptoms, history of previously known chronic complications, laboratory and radiological examinations, and diagnosis made by the physicians. Additionally, if any, other tests were used for diagnosis such as treadmill stress test and coronary arteries calcium scoring for CAD; ankle-to-brachial index of ≤0.9 and limb vessels stenosis of ≥50% on doppler ultrasound for peripheral artery disease; non-mydriatic funduscopy for retinopathy; 10 g monofilament test and 128 Hz tuning fork test for neuropathy; presence of micro-/macroalbuminuria or proteinuria and glomerular filtration rate ≤60 mL/min for DKD; echocardiography for diastolic dysfunction and HF.
Results were presented in n (%), and median (interquartile range, IQR) depends on data type. Chi-squared test was used to compare nominal data, while Mann–Whitney was used to compare numerical data. Logistic regression analysis was used to determine FH+ association with chronic complications adjusted for age, sex, DM duration, alcohol and smoking history, systolic and diastolic blood pressure, body mass index, HbA1c, low-density lipoprotein, triglyceride, and estimated glomerular filtration rate, with no family history of diabetes (FH−) as the reference.
A total of 1011 T2DM patients were included, 24.8% of whom had family history of T2DM (FH+) (Table 1). There were higher proportions of dyslipidemia, smoking and alcohol history found in FH+, whereas FH− had older age, higher systolic blood pressure and triglyceride level, and lower eGFR (Table 1).
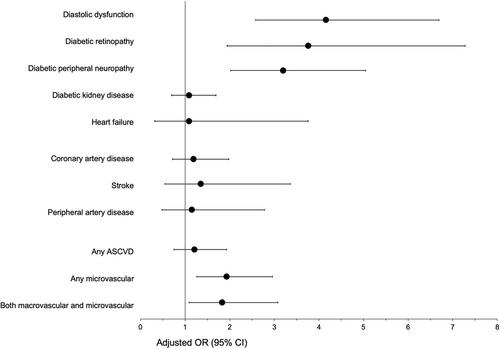
Overall, higher proportions of complications were seen in FH+, but statistical significances were mainly for microvascular complications, not for ASCVD (Figure 1). In multivariate analysis, FH+ remained significantly associated with diastolic dysfunction (adjusted odds ratio [aOR]: 4.16 [2.58–6.69]), retinopathy (aOR: 3.76 [1.94–7.28]), peripheral neuropathy (aOR: 3.20 [2.02–5.05]), composite microvascular complications (aOR: 1.93 [1.26–2.96]), and composite macro- and micro-vascular complications (aOR: 1.83 [1.09–3.08]) (Figure 2).
In this study, we observed a higher proportion of dyslipidemia and a history of smoking and alcohol in FH+ compared to those in FH− group. Nevertheless, having a family history of diabetes was independently associated with increased risks of developing chronic complications, especially diastolic dysfunction, retinopathy, and peripheral neuropathy.
Despite some statistically significant differences in baseline characteristics between FH+ and FH− subjects, it was of no clinical significance. Indeed, we noticed that FH+ patients in our study tended to drink alcohol and smoke in comparison to those in FH− groups. This might contribute to a higher prevalence of dyslipidemia6 in FH+, in addition to the known increased risk of dyslipidemia possessed by having a family history of diabetes.1, 2
FH+ was independently associated with microvascular complications (retinopathy and neuropathy), but not with any ASCVD. In line with previous studies, FH+ was associated with retinopathy and neuropathy but not with DKD7-10; and that family history of CAD or stroke were stronger predictors for ASCVD than family history of diabetes.10-12
FH+ has been associated with younger onset of diabetes, which was characterized by poor glycemic control and more progressive complications.13, 14 Offspring of T2DM has been reported to demonstrate oxidative stress upregulation following high-carbohydrate challenge, in addition to dysregulated antioxidative status, compared to those in the FH- counterpart with similar metabolic profile.15, 16
Previous studies observed that systolic blood pressure was associated with an increased risk of diastolic dysfunction.17, 18 Interestingly, in our study, we found that FH+ was independent predictor of diastolic dysfunction despite lower systolic blood pressure compared to those of FH–. Based on our multivariate analysis, it seems that FH+ impact on diastolic dysfunction surpassed that of systolic blood pressure. On further analysis, both groups had similar proportions of patients having systolic blood pressure under 140 mmHg (61.6% vs. 54.2%, p = 0.055) and 130 mmHg (37.9% vs. 32.1%, p = 0.113), implicating that clinically both groups had similar blood pressure control which might also explain our findings. The mechanism by which FH+ was at higher risk of diastolic dysfunction might be due to impaired cardiac endothelial glycocalyx, autonomic function and relaxation performance.16, 19
Prior hyperglycemic exposure was reported to have long-term effect, called “metabolic memory.”20 Patients with FH+, who were associated with younger onset age and poor glycemic control,14 might be disadvantaged from metabolic memory. Epigenetic mechanisms have been thought of as the contributing factor.20
The unavailability of data regarding age of DM onset and socioeconomic status was one of the limitations of this study. Additionally, retrospective data extraction resulted in some missing examination results. Further research investigating whether FH+ has different epigenetic mechanisms, compared to FH−, as response to similar environmental and metabolic factors is yet to be explored.
In conclusion, T2DM patients with a family history of diabetes had an increased risk for having diastolic dysfunction and microvascular complications. While in the clinical setting this should imply a more rigorous management for this group of patients, in terms of research, further studies are needed to unravel the underlying mechanism.
All authors participated in the conceptualization, methodology, and interpretation of study results. Christian Tricaesario conducted the investigation. William Djauhari and Afif H. Maruf organized data curation. Christian Tricaesario, William Djauhari, and Afif H. Maruf wrote the original draft. Christian Tricaesario did the formal analysis and prepared the visualization of the study results. Dicky L. Tahapary critically reviewed the study, advised on analysis, the visualization of study results, data interpretation, and revised the manuscript. Syahidatul Wafa, Felix F. Widjaja, Jimmy Tandradynata, Rudy Kurniawan, and Muhammad Yamin critically reviewed the article. Sidartawan Soegondo supervised, critically reviewed, and validated the study. All authors have approved the final manuscript.
The authors declare no conflict of interest.
This study was approved by the Ethics Committee of the Faculty of Medicine Universitas Indonesia.
期刊介绍:
This journal aims to promote progress from basic research to clinical practice and to provide a forum for communication among basic, translational, and clinical research practitioners and physicians from all relevant disciplines. Chronic diseases such as cardiovascular diseases, cancer, diabetes, stroke, chronic respiratory diseases (such as asthma and COPD), chronic kidney diseases, and related translational research. Topics of interest for Chronic Diseases and Translational Medicine include Research and commentary on models of chronic diseases with significant implications for disease diagnosis and treatment Investigative studies of human biology with an emphasis on disease Perspectives and reviews on research topics that discuss the implications of findings from the viewpoints of basic science and clinical practic.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
