Holly Morgan, Aish Sinha, Margaret Mcentegart, Suzanna Marie Hardman, Divaka Perera
{"title":"Evaluation of the causes of sex disparity in heart failure trials.","authors":"Holly Morgan, Aish Sinha, Margaret Mcentegart, Suzanna Marie Hardman, Divaka Perera","doi":"10.1136/heartjnl-2021-320696","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Cardiovascular disease is one of the leading causes of mortality and morbidity in women. Despite this, even in contemporary research, female patients are poorly represented in trials. This study aimed to explore reasons behind the sex disparity in heart failure (HF) trials.</p><p><strong>Methods: </strong>HF trials published in seven high-impact clinical journals (impact factor >20), between 2000 and 2020, were identified. Trials with over 300 participants of both sexes were included. Large HF registries, as well as population statistics, were also identified using the same criteria.</p><p><strong>Results: </strong>We identified 146 HF trials, which included 248 620 patients in total. The median proportion of female patients was 25.8%, with the lowest proportions seen in trials enrolling patients with ischaemic cardiomyopathy (17.9%), severe systolic dysfunction (left ventricular ejection fraction (LVEF) <35%) (21.4%) and those involving an invasive procedure (21.1%). The highest proportion of women was seen in trials assessing HF with preserved LVEF (51.6%), as well as trials including older participants (40.5%). Significant differences were seen between prevalence of female trial participants and population prevalence in all LVEF categories (25.8% vs 49.0%, p<0.01).</p><p><strong>Conclusions: </strong>A significant sex disparity was identified in HF trials, most visible in trials assessing patients with severely reduced LVEF and ischaemic aetiology. This is likely due to a complex interplay between enrolment bias and biological variation. Furthermore, the degree of both these aspects may vary according to trial type. Going forward, we should encourage all HF trials to appraise their recruitment log and suggest reasons for any reported sex disparity.</p>","PeriodicalId":9311,"journal":{"name":"British Heart Journal","volume":"108 1","pages":"1547-1552"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9484380/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"British Heart Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/heartjnl-2021-320696","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Cardiovascular disease is one of the leading causes of mortality and morbidity in women. Despite this, even in contemporary research, female patients are poorly represented in trials. This study aimed to explore reasons behind the sex disparity in heart failure (HF) trials.
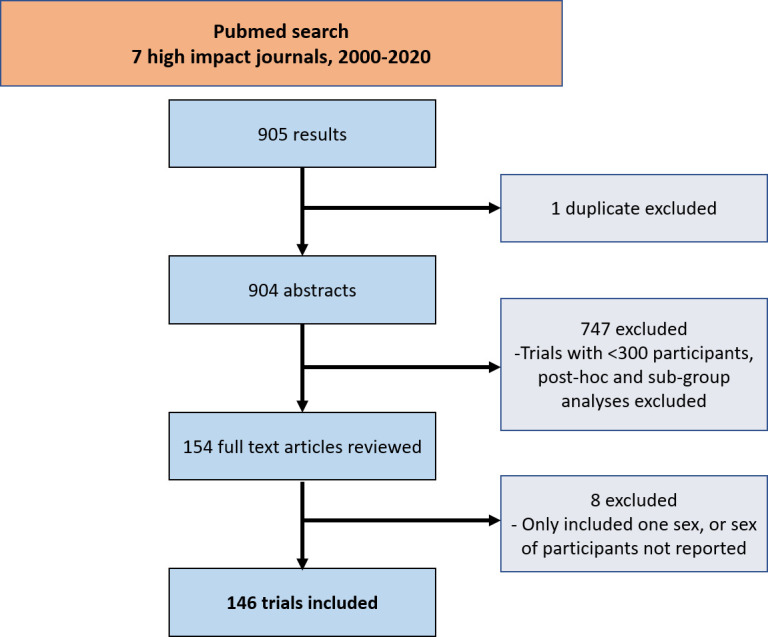
Methods: HF trials published in seven high-impact clinical journals (impact factor >20), between 2000 and 2020, were identified. Trials with over 300 participants of both sexes were included. Large HF registries, as well as population statistics, were also identified using the same criteria.
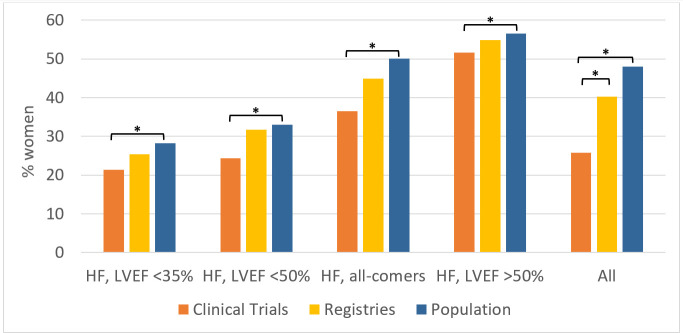
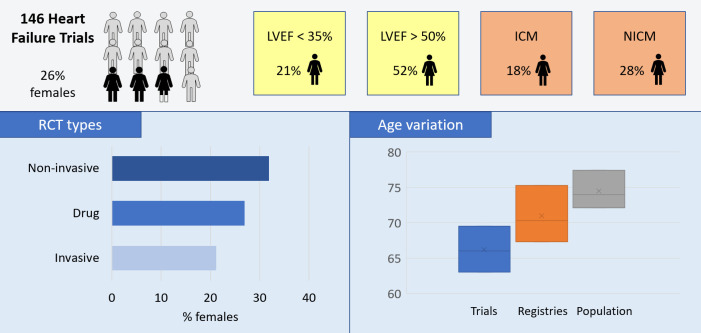
Results: We identified 146 HF trials, which included 248 620 patients in total. The median proportion of female patients was 25.8%, with the lowest proportions seen in trials enrolling patients with ischaemic cardiomyopathy (17.9%), severe systolic dysfunction (left ventricular ejection fraction (LVEF) <35%) (21.4%) and those involving an invasive procedure (21.1%). The highest proportion of women was seen in trials assessing HF with preserved LVEF (51.6%), as well as trials including older participants (40.5%). Significant differences were seen between prevalence of female trial participants and population prevalence in all LVEF categories (25.8% vs 49.0%, p<0.01).
Conclusions: A significant sex disparity was identified in HF trials, most visible in trials assessing patients with severely reduced LVEF and ischaemic aetiology. This is likely due to a complex interplay between enrolment bias and biological variation. Furthermore, the degree of both these aspects may vary according to trial type. Going forward, we should encourage all HF trials to appraise their recruitment log and suggest reasons for any reported sex disparity.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
