Sarah Lanham, Ahmed Maiter, Andrew J Swift, Krit Dwivedi, Samer Alabed, Oscar Evans, Michael J Sharkey, Suzanne Matthews, Christopher S Johns
{"title":"The reproducibility of manual RV/LV ratio measurement on CT pulmonary angiography.","authors":"Sarah Lanham, Ahmed Maiter, Andrew J Swift, Krit Dwivedi, Samer Alabed, Oscar Evans, Michael J Sharkey, Suzanne Matthews, Christopher S Johns","doi":"10.1259/bjro.20220041","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Right ventricular (RV) dysfunction carries elevated risk in acute pulmonary embolism (PE). An increased ratio between the size of the right and left ventricles (RV/LV ratio) is a biomarker of RV dysfunction. This study evaluated the reproducibility of RV/LV ratio measurement on CT pulmonary angiography (CTPA).</p><p><strong>Methods: </strong>20 inpatient CTPA scans performed to assess for acute PE were retrospectively identified from a tertiary UK centre. Each scan was evaluated by 14 radiologists who provided a qualitative overall opinion on the presence of RV dysfunction and measured the RV/LV ratio. Using a threshold of 1.0, the RV/LV ratio measurements were classified as positive (≥1.0) or negative (<1.0) for RV dysfunction. Interobserver agreement was quantified using the Fleiss κ and intraclass correlation coefficient (ICC).</p><p><strong>Results: </strong>Qualitative opinion of RV dysfunction showed weak agreement (κ = 0.42, 95% CI 0.37-0.46). The mean RV/LV ratio measurement for all cases was 1.28 ± 0.68 with significant variation between reporters (<i>p</i> < 0.001). Although agreement for RV/LV measurement was good (ICC = 0.83, 95% CI 0.73-0.91), categorisation of RV dysfunction according to RV/LV ratio measurements showed weak agreement (κ = 0.46, 95% CI 0.41-0.50).</p><p><strong>Conclusion: </strong>Both qualitative opinion and quantitative manual RV/LV ratio measurement show poor agreement for identifying RV dysfunction on CTPA.</p><p><strong>Advances in knowledge: </strong>Caution should be exerted if using manual RV/LV ratio measurements to inform clinical risk stratification and management decisions.</p>","PeriodicalId":72419,"journal":{"name":"BJR open","volume":"1 1","pages":"20220041"},"PeriodicalIF":2.1000,"publicationDate":"2022-11-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10941330/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1259/bjro.20220041","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
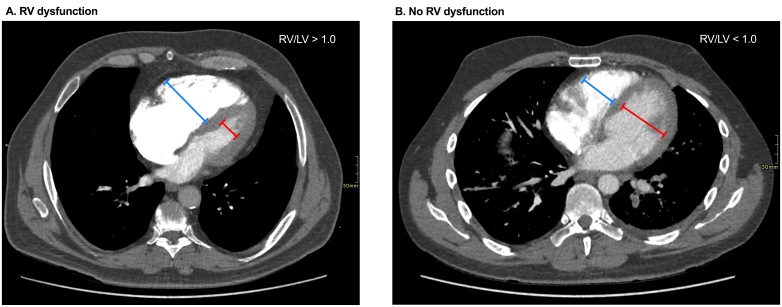
Objectives: Right ventricular (RV) dysfunction carries elevated risk in acute pulmonary embolism (PE). An increased ratio between the size of the right and left ventricles (RV/LV ratio) is a biomarker of RV dysfunction. This study evaluated the reproducibility of RV/LV ratio measurement on CT pulmonary angiography (CTPA).
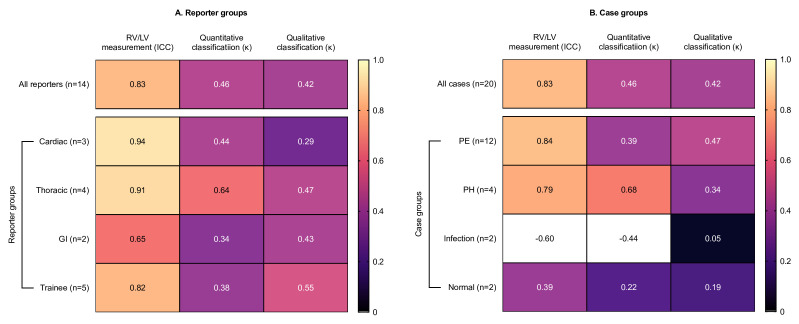
Methods: 20 inpatient CTPA scans performed to assess for acute PE were retrospectively identified from a tertiary UK centre. Each scan was evaluated by 14 radiologists who provided a qualitative overall opinion on the presence of RV dysfunction and measured the RV/LV ratio. Using a threshold of 1.0, the RV/LV ratio measurements were classified as positive (≥1.0) or negative (<1.0) for RV dysfunction. Interobserver agreement was quantified using the Fleiss κ and intraclass correlation coefficient (ICC).
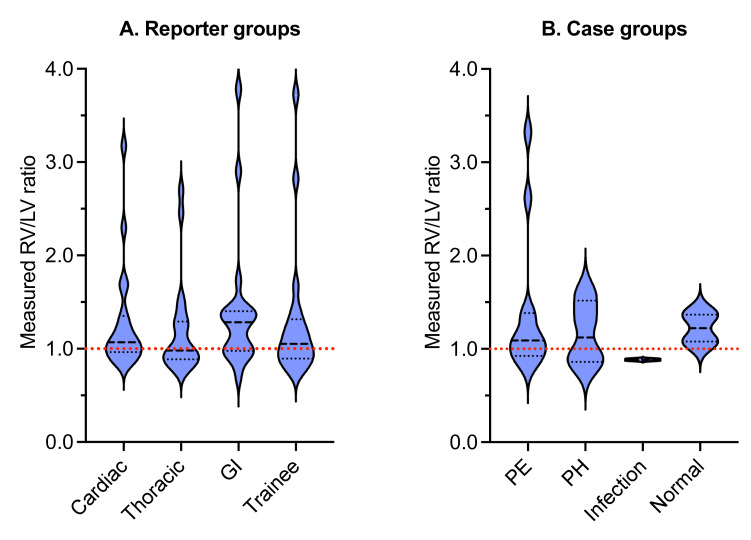
Results: Qualitative opinion of RV dysfunction showed weak agreement (κ = 0.42, 95% CI 0.37-0.46). The mean RV/LV ratio measurement for all cases was 1.28 ± 0.68 with significant variation between reporters (p < 0.001). Although agreement for RV/LV measurement was good (ICC = 0.83, 95% CI 0.73-0.91), categorisation of RV dysfunction according to RV/LV ratio measurements showed weak agreement (κ = 0.46, 95% CI 0.41-0.50).
Conclusion: Both qualitative opinion and quantitative manual RV/LV ratio measurement show poor agreement for identifying RV dysfunction on CTPA.
Advances in knowledge: Caution should be exerted if using manual RV/LV ratio measurements to inform clinical risk stratification and management decisions.
右心室(RV)功能障碍会增加急性肺栓塞(PE)的风险。右心室和左心室大小之间的比率(RV/LV比率)增加是RV功能障碍的生物标志物。本研究评估了CT肺动脉造影(CTPA)中RV/LV比值测量的可重复性。从英国一家三级中心对20名住院患者进行CTPA扫描以评估急性PE进行了回顾性鉴定。每次扫描都由14名放射科医生进行评估,他们对RV功能障碍的存在提供了定性的总体意见,并测量了RV/LV比率。使用1.0的阈值,RV/LV比率测量被分为RV功能障碍的阳性(≥1.0)或阴性(<1.0)。使用κ(κ)和组内相关系数(ICC)量化观察者之间的一致性。RV功能障碍的定性意见显示弱一致性(κ=0.42,95% CI 0.37–0.46)。所有病例的平均RV/LV比值测量值为1.28±0.68,报告者之间存在显著差异(p<0.001)。尽管RV/LV测量值一致性良好(ICC=0.83,95% CI 0.73–0.91),根据RV/LV比率测量对RV功能障碍的分类显示出微弱的一致性(κ=0.46,95% CI 0.41–0.50)。定性意见和定量手动RV/LV比值测量显示,在CTPA上识别RV功能障碍的一致性较差。如果使用手动RV/LV比率测量来告知临床风险分层和管理决策,则应注意。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
