{"title":"A rare etiology of esophageal perforation","authors":"Chih-Chi Tsai, Yen-Chun Peng, Chia-Chang Chen","doi":"10.1002/aid2.13323","DOIUrl":null,"url":null,"abstract":"<p>A 74-year-old male with a history of diabetes and Parkinson's disease presented to our hospital due to progressive dysphagia for 3 months. He also had frequent choking and been admitted to another hospital due to pneumonia before visiting our hospital. He had a surgery of anterior cervical discectomy and fusion (ACDF) 16 years ago due to osteomyelitis with myeloradiculopathy. Cervical roentgenograms showed migrated plate-locking screws, indicating malposition of fixation screw over C7-T1 (Figure 1A). Esophagogastroduodenoscopy was performed to assess the progressive dysphagia (Figure 2).</p><p>What is the diagnosis of this patient?</p><p>The esophagogastroduodenoscopy revealed a screw head had eroded into the esophageal lumen. The exam was stopped promptly to avoid possible complications due to air inflation. Computed tomography of the neck disclosed focal gas accumulation in the esophagus at the C7 level just anterior to the plate. The screw had penetrated through to the esophageal lumen (Figure 1B).</p><p>The incidence of esophageal perforation after ACDF was low (<1%).<span><sup>1</sup></span> The symptoms of esophageal perforation after ACDF includes dysphagia (57%), neck swelling and/or discharge (21%), pneumonia (11%), odynophagia, sore throat (7%), hoarseness, and breathing difficulty (7%).<span><sup>2</sup></span> The diagnosis of esophageal perforation related to ACDF is based on esophagogastroduodenoscopy, upper gastrointestinal series, or esophagogram.</p><p>Most delayed pharyngoesophageal perforations occurred less than 1 year from the time of ACDF. Vrouenraets reported a case of esophageal perforation 9 years post-ACDF with a background of chronic esophagitis.<span><sup>3</sup></span> Our patient experienced this complication 16 years after the surgery. This time frame is the longest ever reported in the literature. Clinicians should consider this differential diagnosis when managing patients with dysphagia and a history of ACDF. Computer tomography or upper GI series should be performed before esophagogastroduodenoscopy if cervical roentgenograms showed malposition of plate-locking screws.</p><p><b>Chia-Chang Chen:</b> The endoscopist who performed the esophagogastroduodenoscopy, final approval and drafting of the manuscript. <b>Chih-Chi Tsai:</b> Final approval and drafting of the manuscript. <b>Yen-Chun Peng:</b> Final approval of the manuscript.</p><p>The authors declare no conflict of interest.</p><p>Written informed consent was obtained from the patient.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"10 2","pages":"125-126"},"PeriodicalIF":0.4000,"publicationDate":"2022-05-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13323","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13323","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
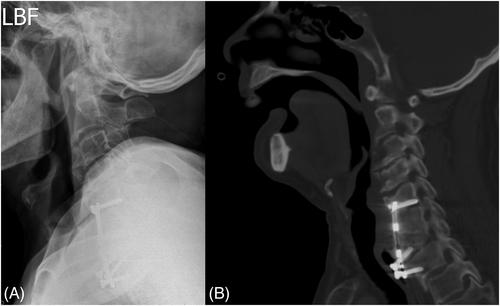
A 74-year-old male with a history of diabetes and Parkinson's disease presented to our hospital due to progressive dysphagia for 3 months. He also had frequent choking and been admitted to another hospital due to pneumonia before visiting our hospital. He had a surgery of anterior cervical discectomy and fusion (ACDF) 16 years ago due to osteomyelitis with myeloradiculopathy. Cervical roentgenograms showed migrated plate-locking screws, indicating malposition of fixation screw over C7-T1 (Figure 1A). Esophagogastroduodenoscopy was performed to assess the progressive dysphagia (Figure 2).
What is the diagnosis of this patient?
The esophagogastroduodenoscopy revealed a screw head had eroded into the esophageal lumen. The exam was stopped promptly to avoid possible complications due to air inflation. Computed tomography of the neck disclosed focal gas accumulation in the esophagus at the C7 level just anterior to the plate. The screw had penetrated through to the esophageal lumen (Figure 1B).
The incidence of esophageal perforation after ACDF was low (<1%).1 The symptoms of esophageal perforation after ACDF includes dysphagia (57%), neck swelling and/or discharge (21%), pneumonia (11%), odynophagia, sore throat (7%), hoarseness, and breathing difficulty (7%).2 The diagnosis of esophageal perforation related to ACDF is based on esophagogastroduodenoscopy, upper gastrointestinal series, or esophagogram.
Most delayed pharyngoesophageal perforations occurred less than 1 year from the time of ACDF. Vrouenraets reported a case of esophageal perforation 9 years post-ACDF with a background of chronic esophagitis.3 Our patient experienced this complication 16 years after the surgery. This time frame is the longest ever reported in the literature. Clinicians should consider this differential diagnosis when managing patients with dysphagia and a history of ACDF. Computer tomography or upper GI series should be performed before esophagogastroduodenoscopy if cervical roentgenograms showed malposition of plate-locking screws.
Chia-Chang Chen: The endoscopist who performed the esophagogastroduodenoscopy, final approval and drafting of the manuscript. Chih-Chi Tsai: Final approval and drafting of the manuscript. Yen-Chun Peng: Final approval of the manuscript.
The authors declare no conflict of interest.
Written informed consent was obtained from the patient.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
