Fereshteh Ghadiri, Omid Mirmosayyeb, Mohammad Ali Sahraian, Abdorreza Naser Moghadasi, Mahsa Ghajarzadeh
{"title":"Alternate dosing of fingolimod in relapsing-remitting multiple sclerosis: A systematic review.","authors":"Fereshteh Ghadiri, Omid Mirmosayyeb, Mohammad Ali Sahraian, Abdorreza Naser Moghadasi, Mahsa Ghajarzadeh","doi":"10.18502/cjn.v22i2.13339","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Fingolimod is approved in relapsing-remitting multiple sclerosis (RRMS) with the recommended dose of 0.5 mg daily. To tackle possible adverse events, some clinicians may reduce the dose of fingolimod, mainly in the alternate-day form. We systematically reviewed the literature for efficacy measures of this method. <b>Methods:</b> PubMed (Medline®), Web of Science, Embase, Scopus, and the Cochrane Library databases were searched until April 9, 2021. Clinical studies (other than case reports and case series), in English, were included. Then, publications concerning alternate dose fingolimod (including every other day, every two or three days) were selected. Those studies concerning reduced daily dose (any daily dose less than 0.5 mg/day) were excluded to focus on alternate dosing. <b>Results:</b> Four observational studies were included. Data on Ohtani et al. study were limited. Three other studies were of good quality based on the Newcastle-Ottawa Scale. A total of 296 patients on the standard dose were compared to 276 patients on the alternate dosage. The most common reason for switching to the alternate dose was lymphopenia, followed by elevated liver enzymes. Two studies concluded that the alternate dosing could be a safe, yet effective strategy in patients with intolerable adverse effects of daily dose. However, Zecca et al. warned about the high possibility of disease reactivation. Due to the differences in outcome measures of the studies, meta-analysis was not applicable. <b>Conclusion:</b> This systematic review highlights the ambiguity of evidence on safety and efficacy of alternate dosing of fingolimod, encouraging further research on the subject.</p>","PeriodicalId":40077,"journal":{"name":"Current Journal of Neurology","volume":"22 1","pages":"110-114"},"PeriodicalIF":0.5000,"publicationDate":"2023-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10460927/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Journal of Neurology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/cjn.v22i2.13339","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
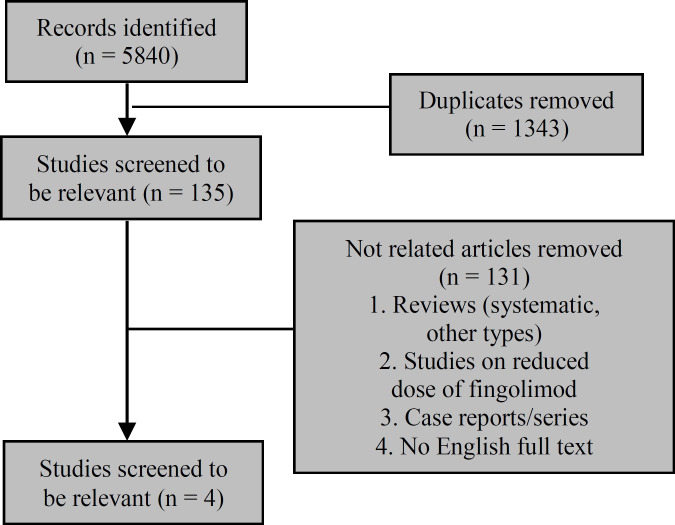
Background: Fingolimod is approved in relapsing-remitting multiple sclerosis (RRMS) with the recommended dose of 0.5 mg daily. To tackle possible adverse events, some clinicians may reduce the dose of fingolimod, mainly in the alternate-day form. We systematically reviewed the literature for efficacy measures of this method. Methods: PubMed (Medline®), Web of Science, Embase, Scopus, and the Cochrane Library databases were searched until April 9, 2021. Clinical studies (other than case reports and case series), in English, were included. Then, publications concerning alternate dose fingolimod (including every other day, every two or three days) were selected. Those studies concerning reduced daily dose (any daily dose less than 0.5 mg/day) were excluded to focus on alternate dosing. Results: Four observational studies were included. Data on Ohtani et al. study were limited. Three other studies were of good quality based on the Newcastle-Ottawa Scale. A total of 296 patients on the standard dose were compared to 276 patients on the alternate dosage. The most common reason for switching to the alternate dose was lymphopenia, followed by elevated liver enzymes. Two studies concluded that the alternate dosing could be a safe, yet effective strategy in patients with intolerable adverse effects of daily dose. However, Zecca et al. warned about the high possibility of disease reactivation. Due to the differences in outcome measures of the studies, meta-analysis was not applicable. Conclusion: This systematic review highlights the ambiguity of evidence on safety and efficacy of alternate dosing of fingolimod, encouraging further research on the subject.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
