Efficacy and safety of different dual antiplatelet strategies in patients undergoing percutaneous coronary intervention: A systematic review and network meta-analysis
{"title":"Efficacy and safety of different dual antiplatelet strategies in patients undergoing percutaneous coronary intervention: A systematic review and network meta-analysis","authors":"Yuttana Wongsalap, Kirati Kengkla, Preyanate Wilairat, Khemanat Ratworawong, Surasak Saokaew, Chaisiri Wanlapakorn","doi":"10.1002/cdt3.85","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Dual antiplatelet therapy (DAPT) is key for preventing ischaemic events post-percutaneous coronary intervention (PCI). Various DAPT modifications like the shortened duration or P2Y12 inhibitor (P2Y12i) de-escalation are implemented to reduce bleeding risk. However, these strategies lack direct comparative studies. This study aimed to assess the efficacy and safety of such DAPT strategies, including de-escalated and short DAPT, in patients undergoing PCI.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We searched PubMed, Embase, Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov databases for relevant randomized controlled trials (RCTs). We performed a network meta-analysis (NMA) to estimate risk ratios (RRs) and 95% confidence intervals (CIs). The primary efficacy endpoint was major adverse cardiac events (MACEs), and the primary safety endpoint was major bleeding. Secondary endpoints included individual components of MACEs and net adverse clinical events (NACEs).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 17 RCTs comprising 53,156 patients (median age, 62.0 years, 24.8% female) were included. NMA suggested that de-escalation DAPT was associated with a significantly lower risk of MACEs (risk ratio [RR] = 0.79, 95% confidence interval [CI] = 0.64–0.98), bleeding (RR = 0.63, 95% CI = 0.49–0.82), and NACEs (RR = 0.69, 95% CI = 0.60–0.79) compared with standard DAPT. Short DAPT followed by P2Y12i monotherapy exhibited a significantly decreased risk of major bleeding (RR = 0.63, 95% CI = 0.46–0.86) compared with standard DAPT.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>De-escalation DAPT was the most effective strategy for preventing the risk of MACEs without increasing bleeding events, while short DAPT followed by P2Y12i monotherapy was the most effective strategy for reducing the risk of bleeding among patients undergoing PCI.</p>\n </section>\n </div>","PeriodicalId":32096,"journal":{"name":"Chronic Diseases and Translational Medicine","volume":"9 4","pages":"299-308"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Diseases and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.85","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Dual antiplatelet therapy (DAPT) is key for preventing ischaemic events post-percutaneous coronary intervention (PCI). Various DAPT modifications like the shortened duration or P2Y12 inhibitor (P2Y12i) de-escalation are implemented to reduce bleeding risk. However, these strategies lack direct comparative studies. This study aimed to assess the efficacy and safety of such DAPT strategies, including de-escalated and short DAPT, in patients undergoing PCI.
Methods
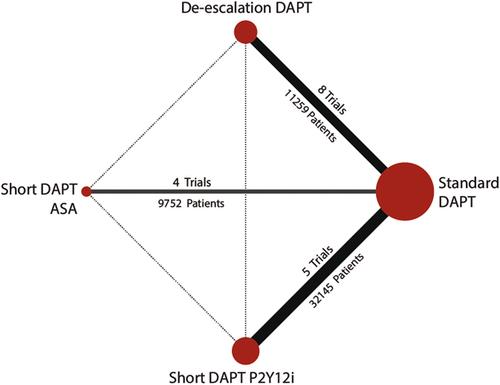
We searched PubMed, Embase, Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov databases for relevant randomized controlled trials (RCTs). We performed a network meta-analysis (NMA) to estimate risk ratios (RRs) and 95% confidence intervals (CIs). The primary efficacy endpoint was major adverse cardiac events (MACEs), and the primary safety endpoint was major bleeding. Secondary endpoints included individual components of MACEs and net adverse clinical events (NACEs).
Results
A total of 17 RCTs comprising 53,156 patients (median age, 62.0 years, 24.8% female) were included. NMA suggested that de-escalation DAPT was associated with a significantly lower risk of MACEs (risk ratio [RR] = 0.79, 95% confidence interval [CI] = 0.64–0.98), bleeding (RR = 0.63, 95% CI = 0.49–0.82), and NACEs (RR = 0.69, 95% CI = 0.60–0.79) compared with standard DAPT. Short DAPT followed by P2Y12i monotherapy exhibited a significantly decreased risk of major bleeding (RR = 0.63, 95% CI = 0.46–0.86) compared with standard DAPT.
Conclusions
De-escalation DAPT was the most effective strategy for preventing the risk of MACEs without increasing bleeding events, while short DAPT followed by P2Y12i monotherapy was the most effective strategy for reducing the risk of bleeding among patients undergoing PCI.
期刊介绍:
This journal aims to promote progress from basic research to clinical practice and to provide a forum for communication among basic, translational, and clinical research practitioners and physicians from all relevant disciplines. Chronic diseases such as cardiovascular diseases, cancer, diabetes, stroke, chronic respiratory diseases (such as asthma and COPD), chronic kidney diseases, and related translational research. Topics of interest for Chronic Diseases and Translational Medicine include Research and commentary on models of chronic diseases with significant implications for disease diagnosis and treatment Investigative studies of human biology with an emphasis on disease Perspectives and reviews on research topics that discuss the implications of findings from the viewpoints of basic science and clinical practic.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
