Rodrigo M Carrillo-Larco, Wilmer Cristobal Guzman-Vilca, Dinesh Neupane
{"title":"Simplified hypertension screening methods across 60 countries: An observational study.","authors":"Rodrigo M Carrillo-Larco, Wilmer Cristobal Guzman-Vilca, Dinesh Neupane","doi":"10.1371/journal.pmed.1003975","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Simplified blood pressure (BP) screening approaches have been proposed. However, evidence is limited to a few countries and has not documented the cardiovascular risk amongst missed hypertension cases, limiting the uptake of these simplified approaches. We quantified the proportion of missed, over-diagnosed, and consistently identified hypertension cases and the 10-year cardiovascular risk in these groups.</p><p><strong>Methods and findings: </strong>We used 60 WHO STEPS surveys (cross-sectional and nationally representative; n = 145,174) conducted in 60 countries in 6 world regions between 2004 and 2019. Nine simplified approaches were compared against the standard (average of the last 2 of 3 BP measurements). The 10-year cardiovascular risk was computed with the 2019 World Health Organization Cardiovascular Risk Charts. We used t tests to compare the cardiovascular risk between the missed and over-diagnosed cases and the consistent hypertension cases. We used Poisson multilevel regressions to identify risk factors for missed cases (adjusted for age, sex, body mass index, and 10-year cardiovascular risk). Across all countries, compared to the standard approach, the simplified approach that missed the fewest cases was using the second BP reading if the first BP reading was 130-145/80-95 mm Hg (5.62%); using only the second BP reading missed 5.82%. The simplified approach with the smallest over-diagnosis proportion was using the second BP reading if the first BP measurement was ≥140/90 mm Hg (3.03%). In many countries, cardiovascular risk was not significantly different between the missed and consistent hypertension groups, yet the mean was slightly lower amongst missed cases. Cardiovascular risk was positively associated with missed hypertension depending on the simplified approach. The main limitation of the work is the cross-sectional design.</p><p><strong>Conclusions: </strong>Simplified BP screening approaches seem to have low misdiagnosis rates, and cardiovascular risk could be lower amongst missed cases than amongst consistent hypertension cases. Simplified BP screening approaches could be included in large screening programmes and busy clinics.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":" ","pages":"e1003975"},"PeriodicalIF":9.9000,"publicationDate":"2022-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9012386/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003975","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Simplified blood pressure (BP) screening approaches have been proposed. However, evidence is limited to a few countries and has not documented the cardiovascular risk amongst missed hypertension cases, limiting the uptake of these simplified approaches. We quantified the proportion of missed, over-diagnosed, and consistently identified hypertension cases and the 10-year cardiovascular risk in these groups.
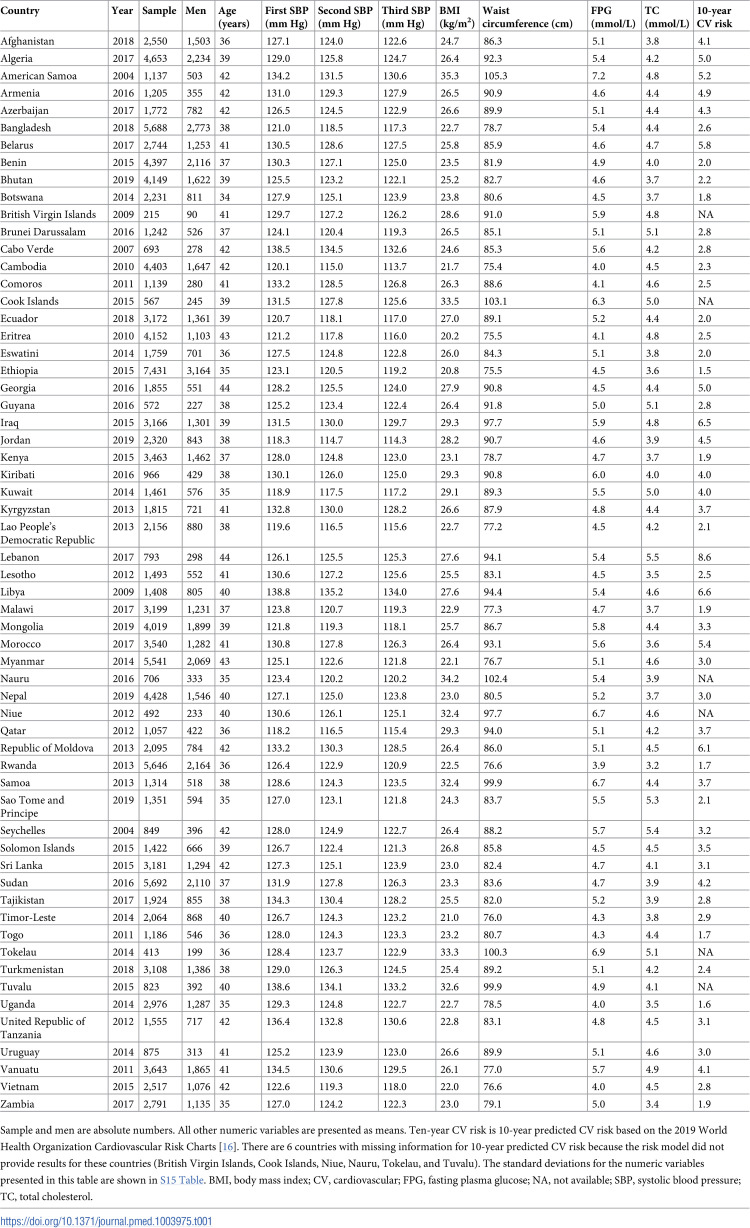
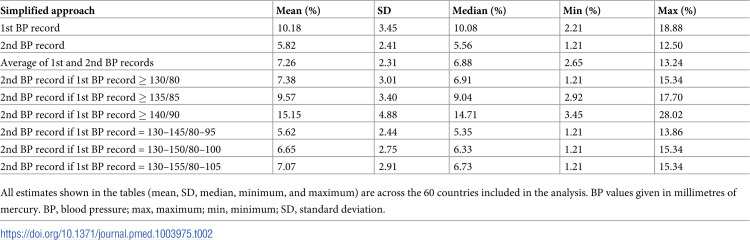
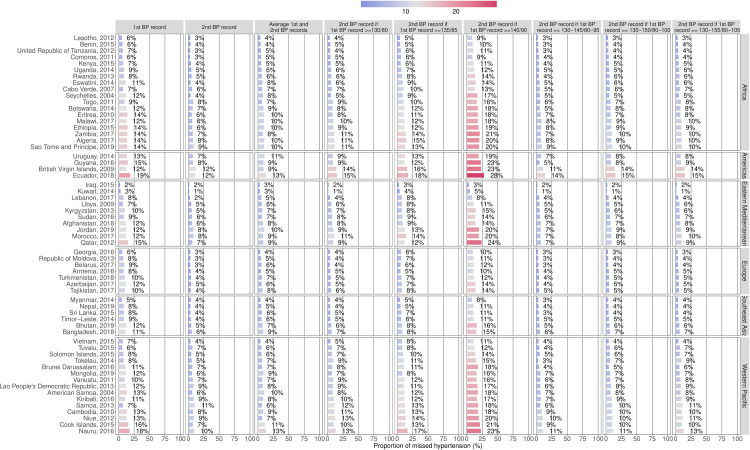
Methods and findings: We used 60 WHO STEPS surveys (cross-sectional and nationally representative; n = 145,174) conducted in 60 countries in 6 world regions between 2004 and 2019. Nine simplified approaches were compared against the standard (average of the last 2 of 3 BP measurements). The 10-year cardiovascular risk was computed with the 2019 World Health Organization Cardiovascular Risk Charts. We used t tests to compare the cardiovascular risk between the missed and over-diagnosed cases and the consistent hypertension cases. We used Poisson multilevel regressions to identify risk factors for missed cases (adjusted for age, sex, body mass index, and 10-year cardiovascular risk). Across all countries, compared to the standard approach, the simplified approach that missed the fewest cases was using the second BP reading if the first BP reading was 130-145/80-95 mm Hg (5.62%); using only the second BP reading missed 5.82%. The simplified approach with the smallest over-diagnosis proportion was using the second BP reading if the first BP measurement was ≥140/90 mm Hg (3.03%). In many countries, cardiovascular risk was not significantly different between the missed and consistent hypertension groups, yet the mean was slightly lower amongst missed cases. Cardiovascular risk was positively associated with missed hypertension depending on the simplified approach. The main limitation of the work is the cross-sectional design.
Conclusions: Simplified BP screening approaches seem to have low misdiagnosis rates, and cardiovascular risk could be lower amongst missed cases than amongst consistent hypertension cases. Simplified BP screening approaches could be included in large screening programmes and busy clinics.
背景:简化的血压(BP)筛查方法已经被提出。然而,证据仅限于少数国家,并没有记录遗漏高血压病例中的心血管风险,限制了这些简化方法的采用。我们量化了这些组中漏诊、过度诊断和一致确定的高血压病例和10年心血管风险的比例。方法和发现我们使用了60项WHO STEPS调查(横断面和全国代表性;N = 145,174),于2004年至2019年在6个世界地区的60个国家进行。将9种简化方法与标准方法(3次BP测量的最后2次的平均值)进行比较。10年心血管风险是根据2019年世界卫生组织心血管风险图表计算的。我们使用t检验比较漏诊和过度诊断病例与一贯高血压病例的心血管风险。我们使用泊松多水平回归来确定漏诊病例的危险因素(调整年龄、性别、体重指数和10年心血管风险)。在所有国家,与标准方法相比,如果第一次血压读数为130-145/80-95 mm Hg,则使用第二次血压读数的简化方法漏报率最少(5.62%);仅使用第二次BP读数就错过了5.82%。如果第一次血压测量≥140/90 mm Hg,则使用第二次血压读数(3.03%)是过度诊断比例最小的简化方法。在许多国家,漏诊组和持续高血压组之间的心血管风险没有显著差异,但漏诊病例的平均值略低。根据简化方法,心血管风险与漏诊高血压呈正相关。该作品的主要限制是截面设计。结论简化血压筛查方法的误诊率较低,漏诊病例的心血管风险低于一致性高血压病例。简化的BP筛查方法可以纳入大型筛查计划和繁忙的诊所。
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
