Katherine A Fu, Russell Kerbel, Rylan J Obrien, Joshua S Li, Nicholas J Jackson, Inna Keselman, Melissa Reider-Demer
{"title":"Optimizing Neurology Inpatient Documentation: A Pilot Study of a Novel Discharge Documentation EHR Tool.","authors":"Katherine A Fu, Russell Kerbel, Rylan J Obrien, Joshua S Li, Nicholas J Jackson, Inna Keselman, Melissa Reider-Demer","doi":"10.1177/19418744231194680","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Clinical documentation of patient acuity is a major determinant of payer reimbursement. This project aimed to improve case mix index (CMI) by incorporating a novel electronic health record (EHR) discharge documentation tool into the inpatient general neurology service at the University of California, Los Angeles (UCLA) Medical Center.</p><p><strong>Methods: </strong>We used data from Vizient AMC Hospital: Risk Model Summary for Clinical Data Base (CBD) 2017 to create a discharge diagnosis documentation tool consisting of dropdown menus to better capture relevant secondary diagnoses and comorbidities. After implementation of this tool, we compared pre- (July 2017-June 2019) and post-intervention (July 2019-June 2021) time periods on mean expected length of stay (LOS) and mean CMI with two sample T-tests and the percentage of encounters classified as having Major Complications/Comorbidities (MCC), with Complication/Comorbidity (CC), and without CC/MCC with tests of proportions.</p><p><strong>Results: </strong>Mean CMI increased significantly from 1.2 pre-intervention to 1.4 post-intervention implementation (<i>P</i> < .01). There was a pattern of increased MCC percentages for \"Bacterial infections,\" \"Other Disorders of Nervous System\", \"Multiple Sclerosis,\" and \"Nervous System Neoplasms\" diagnosis related groups post-intervention.</p><p><strong>Conclusions: </strong>This pilot study describes the creation of an innovative EHR discharge diagnosis documentation tool in collaboration with neurology healthcare providers, the clinical documentation improvement team, and neuro-informaticists. This novel discharge diagnosis documentation tool demonstrates promise in increasing CMI, shifting diagnosis related groups to a greater proportion of those with MCC, and improving the quality of clinical documentation.</p>","PeriodicalId":0,"journal":{"name":"","volume":" ","pages":"5-12"},"PeriodicalIF":0.0,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10790608/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/19418744231194680","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/4 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and purpose: Clinical documentation of patient acuity is a major determinant of payer reimbursement. This project aimed to improve case mix index (CMI) by incorporating a novel electronic health record (EHR) discharge documentation tool into the inpatient general neurology service at the University of California, Los Angeles (UCLA) Medical Center.
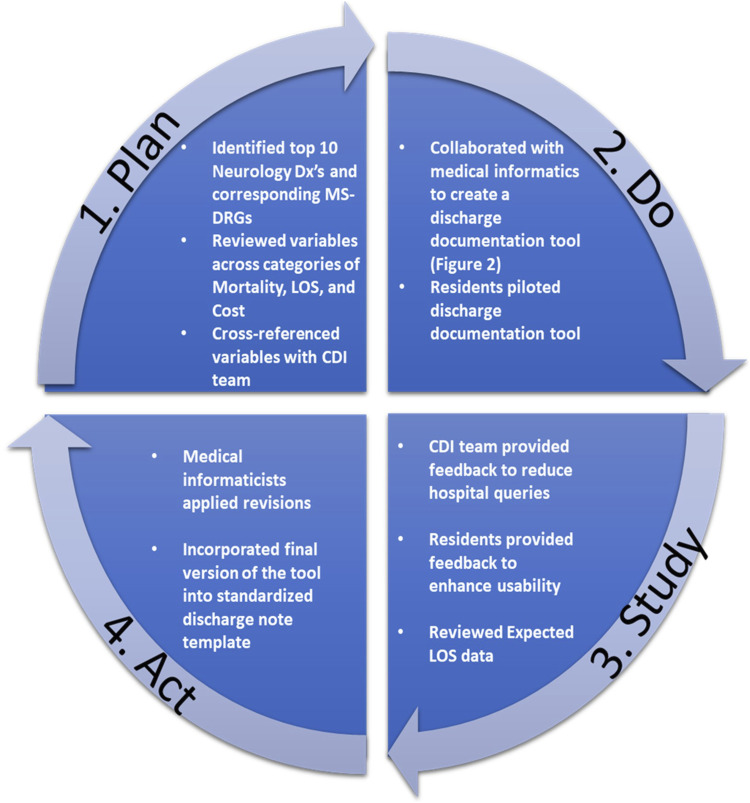
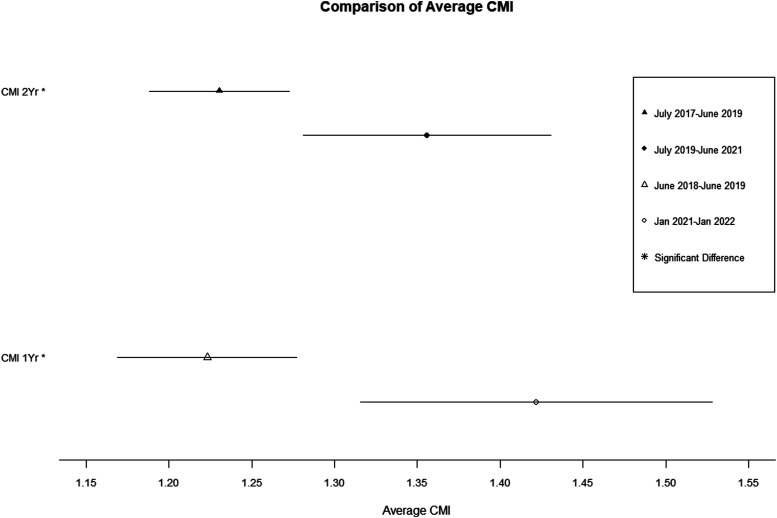
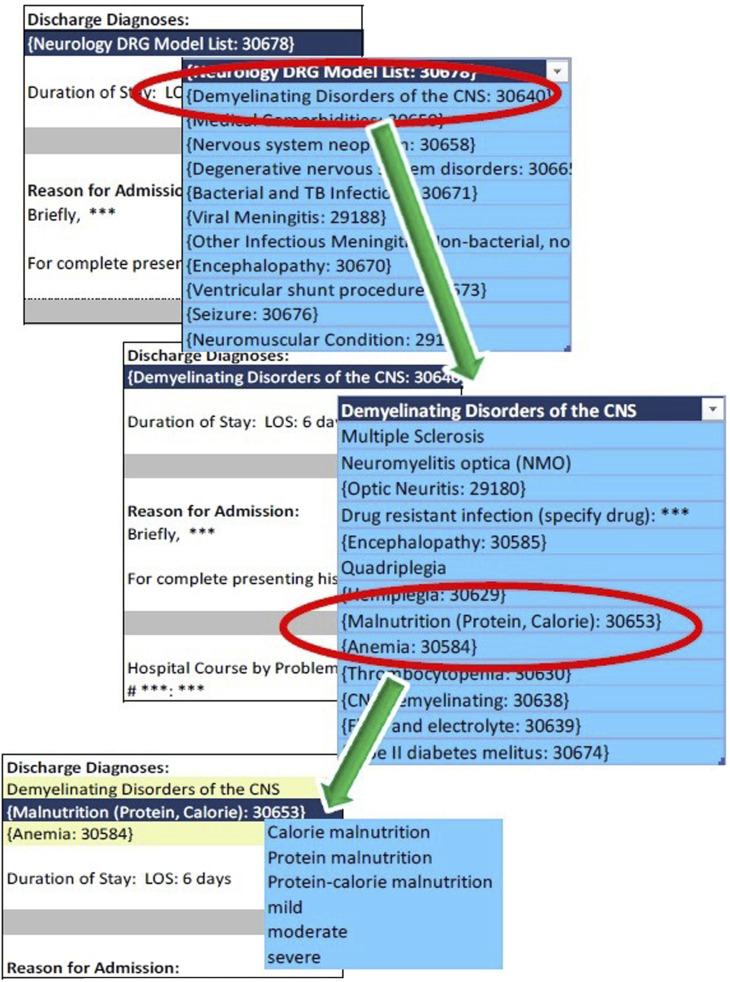
Methods: We used data from Vizient AMC Hospital: Risk Model Summary for Clinical Data Base (CBD) 2017 to create a discharge diagnosis documentation tool consisting of dropdown menus to better capture relevant secondary diagnoses and comorbidities. After implementation of this tool, we compared pre- (July 2017-June 2019) and post-intervention (July 2019-June 2021) time periods on mean expected length of stay (LOS) and mean CMI with two sample T-tests and the percentage of encounters classified as having Major Complications/Comorbidities (MCC), with Complication/Comorbidity (CC), and without CC/MCC with tests of proportions.
Results: Mean CMI increased significantly from 1.2 pre-intervention to 1.4 post-intervention implementation (P < .01). There was a pattern of increased MCC percentages for "Bacterial infections," "Other Disorders of Nervous System", "Multiple Sclerosis," and "Nervous System Neoplasms" diagnosis related groups post-intervention.
Conclusions: This pilot study describes the creation of an innovative EHR discharge diagnosis documentation tool in collaboration with neurology healthcare providers, the clinical documentation improvement team, and neuro-informaticists. This novel discharge diagnosis documentation tool demonstrates promise in increasing CMI, shifting diagnosis related groups to a greater proportion of those with MCC, and improving the quality of clinical documentation.
 分享
分享


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
