Autologous Stem Cell Collection after Daratumumab, Bortezomib, Thalidomide, and Dexamethasone versus Bortezomib, Cyclophosphamide, and Dexamethasone in Newly Diagnosed Multiple Myeloma.
{"title":"Autologous Stem Cell Collection after Daratumumab, Bortezomib, Thalidomide, and Dexamethasone versus Bortezomib, Cyclophosphamide, and Dexamethasone in Newly Diagnosed Multiple Myeloma.","authors":"Sandra Sauer, Katharina Kriegsmann, Cathleen Nientiedt, Anita Schmitt, Carsten Müller-Tidow, Marc-Steffen Raab, Joseph Kauer","doi":"10.1159/000529691","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In transplant-eligible, newly diagnosed multiple myeloma (NDMM) patients, autologous peripheral blood stem cell (PBSC) collection is usually pursued after induction therapy. While induction regimens are constantly refined regarding response, their impact on PBSC collection is not fully studied. The inclusion of the anti-CD38 antibody daratumumab into induction therapy significantly improved outcomes for patients with NDMM, e.g., as part of the daratumumab, bortezomib, thalidomide, and dexamethasone (Dara-VTD) protocol. Preliminary data from the phase 3 CASSIOPEIA study proved the efficacy of Dara-VTD. While overall PBSC collection upon addition of daratumumab was reduced in the study population, more detailed analyses on the impact are missing.</p><p><strong>Methods: </strong>We here report on PBSC mobilization and collection metrics in <i>n</i> = 119 patients with NDMM who underwent induction therapy with bortezomib, cyclophosphamide, and dexamethasone (VCD, <i>n</i> = 61) or Dara-VTD (<i>n</i> = 58).</p><p><strong>Results: </strong>Patient characteristics were well balanced between groups. The Dara-VTD group showed improved response parameters with 66% of patients reaching at least very good partial response versus 54% in the VCD group. Dara-VTD patients exhibited inferior mobilization metrics such as peripheral blood CD34<sup>+</sup> cell count at the first leukapheresis (LP) session (65 vs. 106/μL, <i>p</i> = 0.001), median number of LP sessions (2 vs. 1, <i>p</i> = 0.001), and PBSC collection at first LP (5.5 vs. 8.3 × 10<sup>6</sup>/kg body weight [bw], <i>p</i> = 0.001). Utilization of plerixafor was slightly higher after Dara-VTD (33% vs. 21% of patients, <i>p</i> = 0.143). The overall PBSC collection result was significantly lower after Dara-VTD (8.4 vs. 9.6 × 10<sup>6</sup>/kg bw, <i>p</i> = 0.026). 78% and 85% of patients successfully collected 3 transplants with ≥2 × 10<sup>6</sup> CD34<sup>+</sup> cells/kg bw in the Dara-VTD and the VCD groups, respectively.</p><p><strong>Conclusion: </strong>In summary, Dara-VTD, possibly due to both anti-CD38 antibody and thalidomide exposure, imposes a limitation on PBSC collection which can be only partly overcome by utilization of plerixafor.</p>","PeriodicalId":75241,"journal":{"name":"","volume":"50 1","pages":"371-381"},"PeriodicalIF":0.0,"publicationDate":"2023-03-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10626396/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000529691","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Introduction: In transplant-eligible, newly diagnosed multiple myeloma (NDMM) patients, autologous peripheral blood stem cell (PBSC) collection is usually pursued after induction therapy. While induction regimens are constantly refined regarding response, their impact on PBSC collection is not fully studied. The inclusion of the anti-CD38 antibody daratumumab into induction therapy significantly improved outcomes for patients with NDMM, e.g., as part of the daratumumab, bortezomib, thalidomide, and dexamethasone (Dara-VTD) protocol. Preliminary data from the phase 3 CASSIOPEIA study proved the efficacy of Dara-VTD. While overall PBSC collection upon addition of daratumumab was reduced in the study population, more detailed analyses on the impact are missing.
Methods: We here report on PBSC mobilization and collection metrics in n = 119 patients with NDMM who underwent induction therapy with bortezomib, cyclophosphamide, and dexamethasone (VCD, n = 61) or Dara-VTD (n = 58).
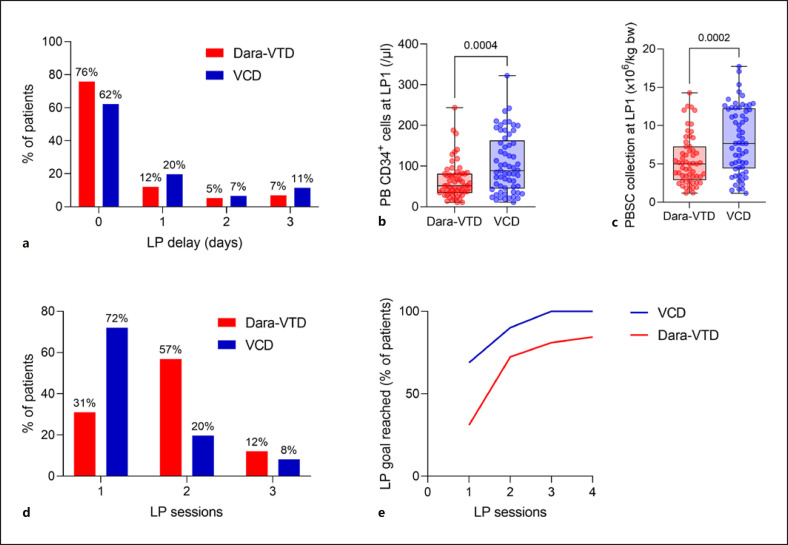
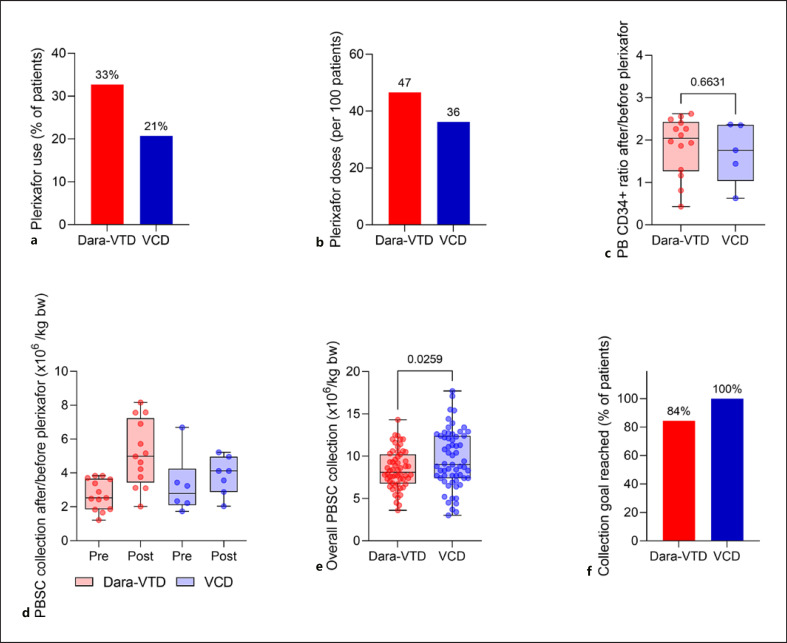
Results: Patient characteristics were well balanced between groups. The Dara-VTD group showed improved response parameters with 66% of patients reaching at least very good partial response versus 54% in the VCD group. Dara-VTD patients exhibited inferior mobilization metrics such as peripheral blood CD34+ cell count at the first leukapheresis (LP) session (65 vs. 106/μL, p = 0.001), median number of LP sessions (2 vs. 1, p = 0.001), and PBSC collection at first LP (5.5 vs. 8.3 × 106/kg body weight [bw], p = 0.001). Utilization of plerixafor was slightly higher after Dara-VTD (33% vs. 21% of patients, p = 0.143). The overall PBSC collection result was significantly lower after Dara-VTD (8.4 vs. 9.6 × 106/kg bw, p = 0.026). 78% and 85% of patients successfully collected 3 transplants with ≥2 × 106 CD34+ cells/kg bw in the Dara-VTD and the VCD groups, respectively.
Conclusion: In summary, Dara-VTD, possibly due to both anti-CD38 antibody and thalidomide exposure, imposes a limitation on PBSC collection which can be only partly overcome by utilization of plerixafor.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
