{"title":"Is the lack of appropriate cognitive demand the primary driver of dementia risk?","authors":"Thomas R. Wood, Josh Turknett","doi":"10.1002/lim2.70","DOIUrl":null,"url":null,"abstract":"<p>With the general trend of increasing lifespan alongside population-level success in reducing the mortality from cardiovascular and cerebrovascular diseases, the population burden of Alzheimer's disease (AD) has steadily accelerated. In the United States, the mortality rate due to AD has increased from less than 0.5 per 100,000 in 1980 to approximately 30 per 100,000 in 2019.<span><sup>1</sup></span> Worldwide, the number of individuals with dementia is expected to at least triple by 2050,<span><sup>2</sup></span> with some reports suggesting that AD has the potential to bankrupt healthcare systems.<span><sup>3</sup></span> At the same time, the development of, and investment in, multiple pharmacological agents directed toward modifying the pathological “hallmarks” of AD have yielded disappointing results. Existing pharmaceuticals offer modest symptomatic benefits, at best, without modifying the course of the disease. Taken together, these factors highlight the urgent need for a critical reappraisal of the underlying risk factors for AD and potential interventions.</p><p>In an attempt to reframe potential preventative and therapeutic approaches to AD, we recently proposed a model that suggests demand–function coupling in the brain is the critical upstream factor driving long-term cognitive function.<span><sup>4</sup></span> In this model, we describe how the health and function of any tissue, including the brain, is shaped by the demands placed upon it. In the setting of increased demand, demand–function coupling drives increases in growth and function, but also upregulates processes of cellular repair and regeneration. The result is a tissue that is more resilient, plastic, and with a greater capacity for increased work output in the face of increased requirements. In this way, we propose that the structure and function of the brain are driven by the demands placed upon it, much as cardiac and skeletal muscles respond to exercise. And as muscle or cardiovascular function decline with bed rest or detraining, the structure and function of the brain decline in a coupled manner when adequate demands are not placed upon it. Cognitive decline is then essentially an expression of “frailty” of the brain - defined as lacking additional capacity to function above basic requirements - as a result of reduced demand. Although it may appear subtle, this reframing of the cascade may be critical in understanding the disease process and intervening as healthcare providers. Whereas the prevailing explanations to date have described cognitive activity as a mitigating force; in this model, we propose that cognitive demand instead impacts the primary pathogenetic process. In fact, given the established phenomenon of demand coupling in neural tissue, we believe that this model provides the most parsimonious account of disease pathogenesis.</p><p>In order to explain the approach, we first made two suggestions for a cognitive framework that we believe are essential if we are to better understand the mechanistic underpinnings of dementia and attempt to intervene in the disease process. The first suggestion was that we should separate late-onset or “sporadic” AD from early-onset familial AD.<span><sup>4</sup></span> Though they both have historically been labeled as forms of AD due to shared neuropathological hallmarks at autopsy, these are completely different diseases with respect to their risk factors and disease course. As such, our model only discusses late-onset AD, which we call age-related dementia (ARD), which is preceded by a period of age-related cognitive decline (ARCD).</p><p>The second suggestion was that we should take an opportunity to explore ARD etiology and intervention points from a different level of biological organization. Every biological phenomenon can be described and characterized at multiple levels of biological organization, from the level of cells and molecules to that of populations and ecosystems.<span><sup>5</sup></span> Every disease phenomenon therefore has a level of analysis and characterization best suited to a coherent explanation of pathogenesis, which is typically the level most upstream in the causal chain. Characterizations of downstream consequences at lower levels of organization, regardless of their level of detail, do not necessarily confer additional or greater explanatory power. In the case of ARD, the field has generally focused on granular, lower level molecular and neuropathological details. This is despite the fact that a growing body of evidence indicates that lifestyle and environment—representing the organismal or societal level of biological organization—are the ultimate level of causation for ARD. If this is truly the case, then interventions at the organismal level are those that are likely to be most impactful, also explaining the general failure (to date) of interventions targeted at the molecular level of AD and ARD.</p><p>One issue with changing the level of organization at which we intervene in a disease process is the fact that it requires us to divest ourselves from thinking purely in terms of well-defined biochemical mechanisms. When developing pharmaceutical agents, it is critical to target a single mechanism while minimizing off-target effects. By comparison, when intervening at the organismal level an intervention may be able to generate powerful results without ever having complete knowledge of its biochemical effects. Indeed, the lack of one single mechanism at the molecular or cellular level of organization has seemed to be a fundamental problem when trying to institute lifestyle medicine at the societal level within medical systems that are singularly focused on the mechanism of action of a given intervention. A good example of this is physical activity, which is perhaps the most impactful single intervention for the treatment and prevention of noncommunicable disease.<span><sup>6</sup></span> Increases in exercise and non-exercise physical activities are uniformly recommended by all government, non-governmental, and health-related organizations despite the fact we are still not entirely sure how physical activity “works.” A number of mechanisms linking physical activity and health, including both acute and chronic functional adaptations to exercise, have been elucidated and documented over several decades. However, even in recent years, we have continued to discover mechanisms by which exercise modulates whole-body health and function, including novel pathways involving irisin, MOTS-c (mitochondrial open reading frame of the 12S rRNA type-c), and Lac-Phe (<i>N</i>-lactoyl-phenylalanine) as just a few examples published in high-impact journals with a large amount of associated press and media interest.<span><sup>7-9</sup></span> If we accept that organismal-level interventions with pleiotropic (and sometimes not fully understood) effects may have the greatest benefit on certain aspects of human health, this allows us to reframe our approach to diseases where few inroads have been made so far, such as ARD.</p><p>When discussing the demand model of ARD with clinicians and researchers with expertise in dementia and neurogenerative conditions, it has not been uncommon for them to ask about other established risk factors, particularly those related to general health and the environment. We must therefore make it very clear that we believe that the environmental component of ARCD and ARD is well-established,<span><sup>10-14</sup></span> and should be an important part of any model for disease etiology or intervention. This includes evidence for significantly increased risk of dementia as well as worse cognitive function associated with reduced physical activity,<span><sup>10, 15-17</sup></span> poor sleep,<span><sup>10, 18, 19</sup></span> metabolic disease,<span><sup>20, 21</sup></span> nutrient deficiencies,<span><sup>14, 22</sup></span> hormonal insufficiency,<span><sup>23</sup></span> altered body composition,<span><sup>24-27</sup></span> and social isolation or poor social support.<span><sup>28</sup></span> Early evidence is also mounting to suggest that lifestyle and environmental modification has the potential to prevent or even reverse ARD, especially when initiated early in the disease process.<span><sup>14, 29, 30</sup></span> A prime example of this is the pioneering work by Prof. David Smith and colleagues, who showed that intervention with B vitamins to lower elevated homocysteine slowed the rate of brain atrophy and cognitive decline, particularly in the setting of adequate omega-3 fatty acid status.<span><sup>22</sup></span> Importantly, the environmental influences on ARD risk map directly to the six evidence-based pillars of lifestyle medicine (Figure 1). We therefore caution against thinking of factors as mutually exclusive, and instead believe the above lifestyle end environmental factors to be critical components required for optimal demand–function coupling in the brain. In order to adapt to increased demand in a tissue, that tissue must also have adequate nutrient availability, hormonal and trophic support, and vascular supply, as well as the absence of toxic exposures and opportunity for sleep recovery and adaptation (e.g., sleep). Insufficiencies in any one of these factors would likely undermine the health-promoting adaptations to cognitive demand. To return to the comparison to exercise, an individual may have all the components required to build healthy muscle tissue—nutrition, hormonal status, sleep, etc.—but in the absence of physical exercise they will not improve their fitness. We believe that all the evidence points to brain function, unsurprisingly, being the same.</p><p>To move beyond the hypothetical, what is the evidence for the primary importance of cognitive demand and what might that mean for the future of AD research and intervention? A recent meta-analysis by Yu et al.<span><sup>14</sup></span> found that cognitive demand late in life was the single most protective factor against AD. Similarly, multiple epidemiological studies suggest that the loss of work-related cognitive stimulus due to retirement results in a parallel increase in the risk of cognitive decline, even after adjusting for confounders that might explain both early retirement and cognitive decline such as comorbid medical conditions.<span><sup>31-33</sup></span> The negative effect of loss of cognitive stimulus is also reversible, as evidenced by increased risk of cognitive decline in those that lose sensory function (e.g., sight, smell, or hearing), which can be overcome by interventions that restore the impaired sense.<span><sup>34-38</sup></span> Other types of beneficial cognitive demand including bilingualism or playing a musical instrument, with greater benefits on brain structure in those for whom the practice is more challenging.<span><sup>39-45</sup></span> Coordinative exercise (e.g., yoga, tai chi, or dancing) also appears to have greater benefits on brain structure and function compared to intensity-matched exercise without a coordination component.<span><sup>46, 47</sup></span> Even structured brain training can have carryover to real-world improvements in memory and executive functions.<span><sup>39, 48-52</sup></span> Although they may initially appear disparate, the upshot of these strands of evidence is that an individual may be able to pick any skill or challenge they are particularly interested in as a way to increase cognitive demands. This would also increase both enjoyment and compliance, as well as making it more likely that these skills may be applied in a social or group setting, which would expectedly provide additional benefits.<span><sup>53</sup></span></p><p>We must acknowledge that limitations exist with the current model and there remains much work to be done in order to determine whether it might help shape the future of interventions for ARD. Cognitive demand is difficult to quantify, and therefore the model is difficult to test. From an implementation standpoint, one might hope that better public awareness of the importance of cognitive demand could drive behavior change and increased cognitive demand at the individual level; however, similar approaches to physical activity have yet to be broadly successful and personalized interventions are likely to be needed.<span><sup>54</sup></span> It is also not yet known whether cognitive demand is both necessary and sufficient to explain ARCD and ARD, and any current attempt to prevent or reverse cognitive decline in a holistic manner should include multi-modal interventions such as those employed in the FINGER (Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability) trial.<span><sup>55</sup></span> This hampers the ability to dissect the relevant contributions of different lifestyle factors, including cognitive demand, on the risk of ARCD and ARD. However, novel trial methodologies could be employed to sequentially alter individual risk factors to determine the relative contributions of cognitive demand.<span><sup>4, 56, 57</sup></span> Additional work could also be done in preclinical experiments such as in rodent models. For instance, we could examine whether the brain is still able to beneficially adapt to increased cognitive demands in the setting of suboptimal nutrient status, general health, or with the presence of toxic exposures such as particulate atmospheric pollution. As an example, work in a mouse model of elevated homocysteine—an important risk factor for AD in humans as mentioned above—found that increased cognitive demand through environmental enrichment was still able to result in beneficial trophic responses in the brain.<span><sup>58</sup></span> If this was the case in a broad range of models of the environmental risk factors for AD in humans, then that would support the proposed model.</p><p>Although there is clearly much to be done, we hope that our demand model of ARD increases awareness and discussion around the importance of cognitive demands for maintaining cognitive function throughout the lifespan. Given that the maintenance of a cognitively active lifestyle has such tremendous promise with virtually zero risks, it is our hope that this model will inspire an enhanced effort to make it a cornerstone of dementia prevention and clinical care, along with research programs to characterize the activities of greatest benefit more thoroughly. Even if proven wrong, we at least hope that people are encouraged in the meantime to dance and sing, and perform more of the critical activities that make us uniquely human, including doing so in social and medical groups with facilitated and peer support.<span><sup>59, 60</sup></span> In the broader sense, this is one of the clearest reasons to implement lifestyle medicine, even if all the mechanistic details remain to be elucidated.</p><p>Dr. Turknett is the founder of Brainjo, a company that creates educational programs for adult learners, and President of Physicians for Ancestral Health. Dr. Wood is a paid scientific advisor for Hintsa Performance, Sidekick Health, Thriva LLC, and Rewire Fitness, and is a founding trustee of the British Society of Lifestyle Medicine.</p><p>The authors received no specific funding for this work.</p>","PeriodicalId":74076,"journal":{"name":"Lifestyle medicine (Hoboken, N.J.)","volume":"3 4","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-10-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lim2.70","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lifestyle medicine (Hoboken, N.J.)","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lim2.70","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
With the general trend of increasing lifespan alongside population-level success in reducing the mortality from cardiovascular and cerebrovascular diseases, the population burden of Alzheimer's disease (AD) has steadily accelerated. In the United States, the mortality rate due to AD has increased from less than 0.5 per 100,000 in 1980 to approximately 30 per 100,000 in 2019.1 Worldwide, the number of individuals with dementia is expected to at least triple by 2050,2 with some reports suggesting that AD has the potential to bankrupt healthcare systems.3 At the same time, the development of, and investment in, multiple pharmacological agents directed toward modifying the pathological “hallmarks” of AD have yielded disappointing results. Existing pharmaceuticals offer modest symptomatic benefits, at best, without modifying the course of the disease. Taken together, these factors highlight the urgent need for a critical reappraisal of the underlying risk factors for AD and potential interventions.
In an attempt to reframe potential preventative and therapeutic approaches to AD, we recently proposed a model that suggests demand–function coupling in the brain is the critical upstream factor driving long-term cognitive function.4 In this model, we describe how the health and function of any tissue, including the brain, is shaped by the demands placed upon it. In the setting of increased demand, demand–function coupling drives increases in growth and function, but also upregulates processes of cellular repair and regeneration. The result is a tissue that is more resilient, plastic, and with a greater capacity for increased work output in the face of increased requirements. In this way, we propose that the structure and function of the brain are driven by the demands placed upon it, much as cardiac and skeletal muscles respond to exercise. And as muscle or cardiovascular function decline with bed rest or detraining, the structure and function of the brain decline in a coupled manner when adequate demands are not placed upon it. Cognitive decline is then essentially an expression of “frailty” of the brain - defined as lacking additional capacity to function above basic requirements - as a result of reduced demand. Although it may appear subtle, this reframing of the cascade may be critical in understanding the disease process and intervening as healthcare providers. Whereas the prevailing explanations to date have described cognitive activity as a mitigating force; in this model, we propose that cognitive demand instead impacts the primary pathogenetic process. In fact, given the established phenomenon of demand coupling in neural tissue, we believe that this model provides the most parsimonious account of disease pathogenesis.
In order to explain the approach, we first made two suggestions for a cognitive framework that we believe are essential if we are to better understand the mechanistic underpinnings of dementia and attempt to intervene in the disease process. The first suggestion was that we should separate late-onset or “sporadic” AD from early-onset familial AD.4 Though they both have historically been labeled as forms of AD due to shared neuropathological hallmarks at autopsy, these are completely different diseases with respect to their risk factors and disease course. As such, our model only discusses late-onset AD, which we call age-related dementia (ARD), which is preceded by a period of age-related cognitive decline (ARCD).
The second suggestion was that we should take an opportunity to explore ARD etiology and intervention points from a different level of biological organization. Every biological phenomenon can be described and characterized at multiple levels of biological organization, from the level of cells and molecules to that of populations and ecosystems.5 Every disease phenomenon therefore has a level of analysis and characterization best suited to a coherent explanation of pathogenesis, which is typically the level most upstream in the causal chain. Characterizations of downstream consequences at lower levels of organization, regardless of their level of detail, do not necessarily confer additional or greater explanatory power. In the case of ARD, the field has generally focused on granular, lower level molecular and neuropathological details. This is despite the fact that a growing body of evidence indicates that lifestyle and environment—representing the organismal or societal level of biological organization—are the ultimate level of causation for ARD. If this is truly the case, then interventions at the organismal level are those that are likely to be most impactful, also explaining the general failure (to date) of interventions targeted at the molecular level of AD and ARD.
One issue with changing the level of organization at which we intervene in a disease process is the fact that it requires us to divest ourselves from thinking purely in terms of well-defined biochemical mechanisms. When developing pharmaceutical agents, it is critical to target a single mechanism while minimizing off-target effects. By comparison, when intervening at the organismal level an intervention may be able to generate powerful results without ever having complete knowledge of its biochemical effects. Indeed, the lack of one single mechanism at the molecular or cellular level of organization has seemed to be a fundamental problem when trying to institute lifestyle medicine at the societal level within medical systems that are singularly focused on the mechanism of action of a given intervention. A good example of this is physical activity, which is perhaps the most impactful single intervention for the treatment and prevention of noncommunicable disease.6 Increases in exercise and non-exercise physical activities are uniformly recommended by all government, non-governmental, and health-related organizations despite the fact we are still not entirely sure how physical activity “works.” A number of mechanisms linking physical activity and health, including both acute and chronic functional adaptations to exercise, have been elucidated and documented over several decades. However, even in recent years, we have continued to discover mechanisms by which exercise modulates whole-body health and function, including novel pathways involving irisin, MOTS-c (mitochondrial open reading frame of the 12S rRNA type-c), and Lac-Phe (N-lactoyl-phenylalanine) as just a few examples published in high-impact journals with a large amount of associated press and media interest.7-9 If we accept that organismal-level interventions with pleiotropic (and sometimes not fully understood) effects may have the greatest benefit on certain aspects of human health, this allows us to reframe our approach to diseases where few inroads have been made so far, such as ARD.
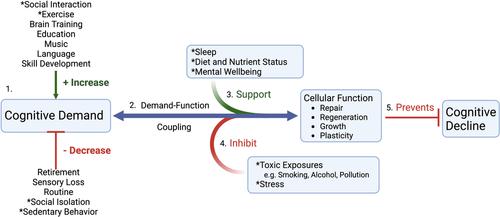
When discussing the demand model of ARD with clinicians and researchers with expertise in dementia and neurogenerative conditions, it has not been uncommon for them to ask about other established risk factors, particularly those related to general health and the environment. We must therefore make it very clear that we believe that the environmental component of ARCD and ARD is well-established,10-14 and should be an important part of any model for disease etiology or intervention. This includes evidence for significantly increased risk of dementia as well as worse cognitive function associated with reduced physical activity,10, 15-17 poor sleep,10, 18, 19 metabolic disease,20, 21 nutrient deficiencies,14, 22 hormonal insufficiency,23 altered body composition,24-27 and social isolation or poor social support.28 Early evidence is also mounting to suggest that lifestyle and environmental modification has the potential to prevent or even reverse ARD, especially when initiated early in the disease process.14, 29, 30 A prime example of this is the pioneering work by Prof. David Smith and colleagues, who showed that intervention with B vitamins to lower elevated homocysteine slowed the rate of brain atrophy and cognitive decline, particularly in the setting of adequate omega-3 fatty acid status.22 Importantly, the environmental influences on ARD risk map directly to the six evidence-based pillars of lifestyle medicine (Figure 1). We therefore caution against thinking of factors as mutually exclusive, and instead believe the above lifestyle end environmental factors to be critical components required for optimal demand–function coupling in the brain. In order to adapt to increased demand in a tissue, that tissue must also have adequate nutrient availability, hormonal and trophic support, and vascular supply, as well as the absence of toxic exposures and opportunity for sleep recovery and adaptation (e.g., sleep). Insufficiencies in any one of these factors would likely undermine the health-promoting adaptations to cognitive demand. To return to the comparison to exercise, an individual may have all the components required to build healthy muscle tissue—nutrition, hormonal status, sleep, etc.—but in the absence of physical exercise they will not improve their fitness. We believe that all the evidence points to brain function, unsurprisingly, being the same.
To move beyond the hypothetical, what is the evidence for the primary importance of cognitive demand and what might that mean for the future of AD research and intervention? A recent meta-analysis by Yu et al.14 found that cognitive demand late in life was the single most protective factor against AD. Similarly, multiple epidemiological studies suggest that the loss of work-related cognitive stimulus due to retirement results in a parallel increase in the risk of cognitive decline, even after adjusting for confounders that might explain both early retirement and cognitive decline such as comorbid medical conditions.31-33 The negative effect of loss of cognitive stimulus is also reversible, as evidenced by increased risk of cognitive decline in those that lose sensory function (e.g., sight, smell, or hearing), which can be overcome by interventions that restore the impaired sense.34-38 Other types of beneficial cognitive demand including bilingualism or playing a musical instrument, with greater benefits on brain structure in those for whom the practice is more challenging.39-45 Coordinative exercise (e.g., yoga, tai chi, or dancing) also appears to have greater benefits on brain structure and function compared to intensity-matched exercise without a coordination component.46, 47 Even structured brain training can have carryover to real-world improvements in memory and executive functions.39, 48-52 Although they may initially appear disparate, the upshot of these strands of evidence is that an individual may be able to pick any skill or challenge they are particularly interested in as a way to increase cognitive demands. This would also increase both enjoyment and compliance, as well as making it more likely that these skills may be applied in a social or group setting, which would expectedly provide additional benefits.53
We must acknowledge that limitations exist with the current model and there remains much work to be done in order to determine whether it might help shape the future of interventions for ARD. Cognitive demand is difficult to quantify, and therefore the model is difficult to test. From an implementation standpoint, one might hope that better public awareness of the importance of cognitive demand could drive behavior change and increased cognitive demand at the individual level; however, similar approaches to physical activity have yet to be broadly successful and personalized interventions are likely to be needed.54 It is also not yet known whether cognitive demand is both necessary and sufficient to explain ARCD and ARD, and any current attempt to prevent or reverse cognitive decline in a holistic manner should include multi-modal interventions such as those employed in the FINGER (Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability) trial.55 This hampers the ability to dissect the relevant contributions of different lifestyle factors, including cognitive demand, on the risk of ARCD and ARD. However, novel trial methodologies could be employed to sequentially alter individual risk factors to determine the relative contributions of cognitive demand.4, 56, 57 Additional work could also be done in preclinical experiments such as in rodent models. For instance, we could examine whether the brain is still able to beneficially adapt to increased cognitive demands in the setting of suboptimal nutrient status, general health, or with the presence of toxic exposures such as particulate atmospheric pollution. As an example, work in a mouse model of elevated homocysteine—an important risk factor for AD in humans as mentioned above—found that increased cognitive demand through environmental enrichment was still able to result in beneficial trophic responses in the brain.58 If this was the case in a broad range of models of the environmental risk factors for AD in humans, then that would support the proposed model.
Although there is clearly much to be done, we hope that our demand model of ARD increases awareness and discussion around the importance of cognitive demands for maintaining cognitive function throughout the lifespan. Given that the maintenance of a cognitively active lifestyle has such tremendous promise with virtually zero risks, it is our hope that this model will inspire an enhanced effort to make it a cornerstone of dementia prevention and clinical care, along with research programs to characterize the activities of greatest benefit more thoroughly. Even if proven wrong, we at least hope that people are encouraged in the meantime to dance and sing, and perform more of the critical activities that make us uniquely human, including doing so in social and medical groups with facilitated and peer support.59, 60 In the broader sense, this is one of the clearest reasons to implement lifestyle medicine, even if all the mechanistic details remain to be elucidated.
Dr. Turknett is the founder of Brainjo, a company that creates educational programs for adult learners, and President of Physicians for Ancestral Health. Dr. Wood is a paid scientific advisor for Hintsa Performance, Sidekick Health, Thriva LLC, and Rewire Fitness, and is a founding trustee of the British Society of Lifestyle Medicine.
The authors received no specific funding for this work.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
