{"title":"Psoriasis-like eruptions developed in an atopic dermatitis patient treated with dupilumab","authors":"Rai Fujimoto MD, Yoko Kataoka MD","doi":"10.1002/cia2.12251","DOIUrl":null,"url":null,"abstract":"<p>Dupilumab is a human monoclonal antibody that binds to the alpha-subunit of interleukin (IL)-4 and IL-13 receptors that play a dominant role in the T-helper (Th)2 cytokine cascade related to atopic dermatitis (AD). Dupilumab is useful in treating moderate to severe AD by inhibiting the signaling of IL-4 and IL-13 without severe adverse effects.<span><sup>1</sup></span> Herein, we report a case of a patient with psoriasis-like eruptions, which developed during treatment with dupilumab.</p><p>The 49-year-old man had a history of AD since childhood. He also had bronchial asthma, allergic rhinitis, and allergic conjunctivitis. Although he was treated with topical medications, he experienced repeated flare-ups of eczema. At the time of presentation, erythema was distributed over the trunk and extremities, with some lichenification. There was also skin atrophy on the extremities. He was diagnosed as having severe AD to the Hanifin-Rajika criteria (eczema area and severity index = 19.2, patient-oriented eczema measure = 28, average numerical rating scale = 10, and dermatology life quality index = 29). After the diagnosis, the treatment with dupilumab started according to the dosage regimen for AD (600 mg as the first dose, followed by 300 mg every 2 weeks). Although overall symptoms showed improvement, the flare-up of erythema was observed with the discontinuation of topical steroids. After 16 months of treatment with dupilumab, the patient was referred to us for exacerbation on the scalp and back. Scattered erythematous and scaly plaques, whose morphology was suggestive of psoriasis, were found on the back and scalp (Figure 1A,B). Histopathological examination revealed parakeratosis and hyperkeratosis and a lack of stratum granulosum (Figure 1C). The diagnosis of psoriasis-like eruptions after dupilumab was made. Although the lesion once improved after topical steroids, narrowband UVB, and oral etretinate 50 mg, the eruptions repeated flare-ups. In addition, the AD lesion has also tended to flare up, and continuation of dupilumab has been necessary.</p><p>Psoriasis vulgaris is a disease considered to be driven by a Th17 cascade, with elevated levels of IL-17 A and IL-23. In contrast, AD is a Th2 cell-mediated disease with elevated IL-4 and IL-13 levels. Although there are some reports on the development of psoriasis-like eruptions during treatment with dupilumab for AD, no reports refer to Asians.<span><sup>2</sup></span> Recent studies have revealed that IL-4 negatively regulates Th1 and Th17 cells.<span><sup>3, 4</sup></span> A study on AD endotypes reported elevated levels of Th17-related cytokines in lesional and nonlesional skin of Asian AD patients compared to those of European AD patients.<span><sup>5</sup></span> Thus, we hypothesize that blocking IL-4 by dupilumab may have caused a relative increase in latent Th17-related inflammation, resulting in psoriasis-like eruptions in our case. Above all, the discontinuation of dupilumab was not necessary to treat psoriasis-like eruptions, which is one of the most notable points in our case. However, the onset of psoriasis-like eruptions in our case was later after the initiation of dupilumab than in other reports. This difference implies that the tendency to relapse AD despite dupilumab treatment delayed the onset of psoriasis-like eruptions. Our case suggests that psoriasis vulgaris could occur during treatment with dupilumab, particularly in Asians, and requires careful follow-up.</p><p>The authors declare no conflict of interest.</p><p>Approval of the research protocol: N/A.</p><p>Informed Consent: N/A.</p><p>Registry and the Registration No. of the study/trial: N/A.</p><p>Animal Studies: N/A.</p>","PeriodicalId":15543,"journal":{"name":"Journal of Cutaneous Immunology and Allergy","volume":"5 6","pages":"231-232"},"PeriodicalIF":0.9000,"publicationDate":"2022-05-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12251","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Immunology and Allergy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12251","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 2
Abstract
Dupilumab is a human monoclonal antibody that binds to the alpha-subunit of interleukin (IL)-4 and IL-13 receptors that play a dominant role in the T-helper (Th)2 cytokine cascade related to atopic dermatitis (AD). Dupilumab is useful in treating moderate to severe AD by inhibiting the signaling of IL-4 and IL-13 without severe adverse effects.1 Herein, we report a case of a patient with psoriasis-like eruptions, which developed during treatment with dupilumab.
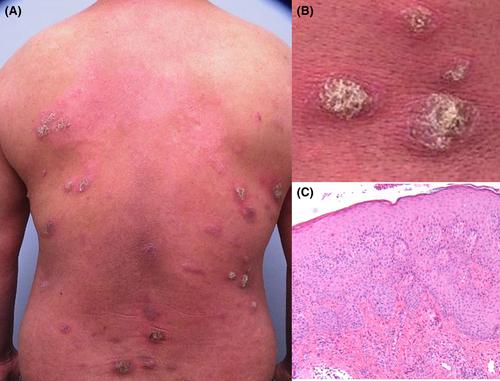
The 49-year-old man had a history of AD since childhood. He also had bronchial asthma, allergic rhinitis, and allergic conjunctivitis. Although he was treated with topical medications, he experienced repeated flare-ups of eczema. At the time of presentation, erythema was distributed over the trunk and extremities, with some lichenification. There was also skin atrophy on the extremities. He was diagnosed as having severe AD to the Hanifin-Rajika criteria (eczema area and severity index = 19.2, patient-oriented eczema measure = 28, average numerical rating scale = 10, and dermatology life quality index = 29). After the diagnosis, the treatment with dupilumab started according to the dosage regimen for AD (600 mg as the first dose, followed by 300 mg every 2 weeks). Although overall symptoms showed improvement, the flare-up of erythema was observed with the discontinuation of topical steroids. After 16 months of treatment with dupilumab, the patient was referred to us for exacerbation on the scalp and back. Scattered erythematous and scaly plaques, whose morphology was suggestive of psoriasis, were found on the back and scalp (Figure 1A,B). Histopathological examination revealed parakeratosis and hyperkeratosis and a lack of stratum granulosum (Figure 1C). The diagnosis of psoriasis-like eruptions after dupilumab was made. Although the lesion once improved after topical steroids, narrowband UVB, and oral etretinate 50 mg, the eruptions repeated flare-ups. In addition, the AD lesion has also tended to flare up, and continuation of dupilumab has been necessary.
Psoriasis vulgaris is a disease considered to be driven by a Th17 cascade, with elevated levels of IL-17 A and IL-23. In contrast, AD is a Th2 cell-mediated disease with elevated IL-4 and IL-13 levels. Although there are some reports on the development of psoriasis-like eruptions during treatment with dupilumab for AD, no reports refer to Asians.2 Recent studies have revealed that IL-4 negatively regulates Th1 and Th17 cells.3, 4 A study on AD endotypes reported elevated levels of Th17-related cytokines in lesional and nonlesional skin of Asian AD patients compared to those of European AD patients.5 Thus, we hypothesize that blocking IL-4 by dupilumab may have caused a relative increase in latent Th17-related inflammation, resulting in psoriasis-like eruptions in our case. Above all, the discontinuation of dupilumab was not necessary to treat psoriasis-like eruptions, which is one of the most notable points in our case. However, the onset of psoriasis-like eruptions in our case was later after the initiation of dupilumab than in other reports. This difference implies that the tendency to relapse AD despite dupilumab treatment delayed the onset of psoriasis-like eruptions. Our case suggests that psoriasis vulgaris could occur during treatment with dupilumab, particularly in Asians, and requires careful follow-up.
The authors declare no conflict of interest.
Approval of the research protocol: N/A.
Informed Consent: N/A.
Registry and the Registration No. of the study/trial: N/A.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
