Allison O. Dumitriu Carcoana , Jenna C. Marek , William J. West III , Cole R. Fiedler , William N. Doyle Jr. , Kristie M. Labib , Lauren C. Ladehoff , Jose A. Malavet , Gregory Fishberger , Carla C. Moodie , Joseph R. Garrett , Jenna R. Tew , Jobelle J.A.R. Baldonado , Jacques P. Fontaine , Eric M. Toloza
{"title":"Residential Distance to the Cancer Center and Outcomes after Robotic-Assisted Pulmonary Lobectomy","authors":"Allison O. Dumitriu Carcoana , Jenna C. Marek , William J. West III , Cole R. Fiedler , William N. Doyle Jr. , Kristie M. Labib , Lauren C. Ladehoff , Jose A. Malavet , Gregory Fishberger , Carla C. Moodie , Joseph R. Garrett , Jenna R. Tew , Jobelle J.A.R. Baldonado , Jacques P. Fontaine , Eric M. Toloza","doi":"10.1016/j.sipas.2023.100210","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Outcomes of lung cancer patients traveling greater distances for surgical oncology care are not well-described. We investigated the effects of increased travel burden after robotic-assisted pulmonary lobectomy (RAPL) for lung cancer.</p></div><div><h3>Methods</h3><p>Clinical characteristics and surgical outcomes of 711 consecutive patients who underwent RAPL from September 2010 to March 2022 were compared, stratified by primary residential ZIP code <160 km or ≥160 km from the cancer center.</p></div><div><h3>Results</h3><p>Of 711 study patients, 515 (72.4%) lived within 160 km and 196 (27.6%) lived ≥160 km away. There were no differences in Charlson Comorbidity Index scores or tumor characteristics. Those traveling ≥160 km experienced more unfavorable perioperative outcomes and postoperative complications, and had worse median survival time by 1.68 years, but this survival difference did not reach statistical significance.</p></div><div><h3>Conclusions</h3><p>With the growing centralization of cancer care, travel burden may emerge as a predictor of surgical oncology outcomes.</p></div>","PeriodicalId":74890,"journal":{"name":"Surgery in practice and science","volume":"15 ","pages":"Article 100210"},"PeriodicalIF":0.8000,"publicationDate":"2023-08-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgery in practice and science","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666262023000566","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
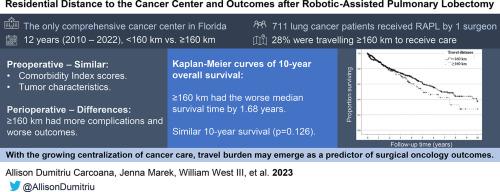
Outcomes of lung cancer patients traveling greater distances for surgical oncology care are not well-described. We investigated the effects of increased travel burden after robotic-assisted pulmonary lobectomy (RAPL) for lung cancer.
Methods
Clinical characteristics and surgical outcomes of 711 consecutive patients who underwent RAPL from September 2010 to March 2022 were compared, stratified by primary residential ZIP code <160 km or ≥160 km from the cancer center.
Results
Of 711 study patients, 515 (72.4%) lived within 160 km and 196 (27.6%) lived ≥160 km away. There were no differences in Charlson Comorbidity Index scores or tumor characteristics. Those traveling ≥160 km experienced more unfavorable perioperative outcomes and postoperative complications, and had worse median survival time by 1.68 years, but this survival difference did not reach statistical significance.
Conclusions
With the growing centralization of cancer care, travel burden may emerge as a predictor of surgical oncology outcomes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
