Repair of abdominal aortic aneurysms (AAA) decreases the incidence of rupture and death. In cancer patients, sarcopenia has been associated with increased surgical complications and mortality. The impact of sarcopenia on survival after AAA repair has yet to be described.
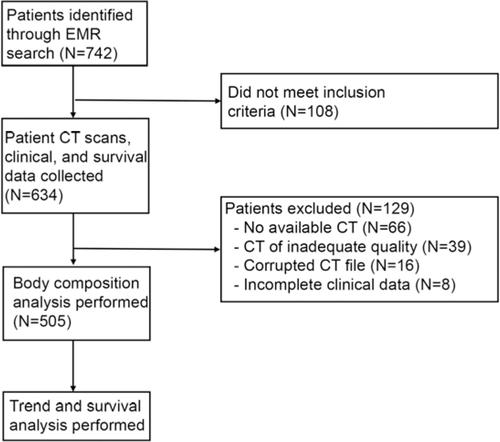
Patient demographic, laboratory, body composition measurements and survival data were obtained from patients undergoing AAA repair at the Indiana University medical campus over a 5-year period. Univariate and multivariate analyses were performed to identify factors associated with overall survival. Overall, 58.2% presented with sarcopenia. Sarcopenic patients were older (71.8±8.3 versus 66.8±8.1 years; p<0.001), had lower body mass index (BMI) (26.3±5.2 versus 31.5±5.9 kg/m2; p<0.001), higher rates of myosteatosis (84.4% versus 52.%; p<0.001), greater AAA diameter (60.6±14.0 versus 57.8±11.7 mm; p=0.016), higher Charlson Comorbidity Index (CCI) (32.3% versus 25.1% ≥6; p=0.034), and increased rates of rupture (8.2% versus 3.8%; p=0.047). Sarcopenic and nonsarcopenic patients had no difference in 30-day morbidity (8.5% versus 8.5%; p=0.991) or mortality (3.7% versus 0.9%; p=0.07). Univariate analysis demonstrated age, sarcopenia, myosteatosis, CCI, and BMI to be associated with long-term survival. There was no correlation between BMI and sarcopenia. Both sarcopenia and myosteatosis resulted in decreased one-, three-, and five-year survivals compared to their counterparts. On multivariate analysis sarcopenia is independently associated with survival, conferring a 1.6-fold increase in death (p=0.04). The combination of sarcopenia plus myosteatosis doubled the risk of death compared to sarcopenia alone.
This is the first study to demonstrate that over half of all patients undergoing AAA repair are sarcopenic, a condition associated with increased mortality. Sarcopenia with myosteatosis is associated with double the mortality of sarcopenia alone. CT scan, but not BMI, accurately identifies sarcopenia and myosteatosis. Defining the mechanisms through which sarcopenia contributes to late death after AAA repair is critical to developing novel interventions that may improve survival in this high risk population.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
