Severe acute respiratory syndrome coronavirus 2 (SARSCoV2) has been associated with several neuro-ophthalmic manifestations. We report a case of bilateral longitudinally extensive optic perineuritis suspected due to SARSCoV2.
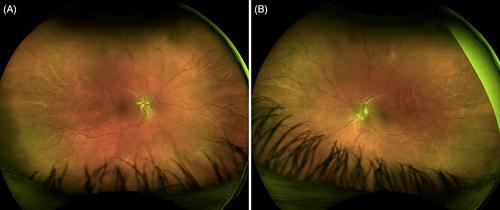
A 32-year-old woman developed headaches, photophobia, pulsatile tinnitus, and blurred vision 8 d after having a positive SARS-CoV-2 qualitative polymerase chain reaction (PCR) testing for coronavirus disease 2019 (COVID-19). She was diagnosed with and treated for idiopathic intracranial hypertension (IIH) elsewhere. Repeat evaluation at our institution showed a poor visual acuity in both eyes with Frisen grade II papilledema and cotton wool spots on fundoscopic examination. Orbital magnetic resonance imaging (MRI) showed bilateral longitudinally extensive optic nerve sheath enhancement. Repeat lumbar puncture revealed an elevated cerebrospinal fluid (CSF) opening pressure and protein, a finding that is incompatible with the diagnosis of IIH. Myelin oligodendrocyte glycoprotein, aquaporin-4 (AQP4)-IgG antibodies, and other serological tests for optic neuritis were unremarkable. Her visual acuity partially improved after corticosteroids. With the growing association of demyelinating disorders and COVID-19, unremarkable serological workup, and temporal relation of the patient's symptoms to the infection, we believe that her diagnosis is SARS-CoV-2 associated bilateral optic neuritis.
There is a growing association between demyelinating disorders and COVID-19 and COVID-19 vaccination, and it is essential to recognize CSF abnormalities that are incompatible with a diagnosis of IIH, such as increased protein in our case, and may lead to an incorrect diagnosis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
