Andrew James Boyle, Peter Ferris, Ian Bradbury, John Conlon, Manu Shankar-Hari, Angela J Rogers, Cecilia M O'Kane, Daniel F McAuley
{"title":"Baseline plasma IL-18 may predict simvastatin treatment response in patients with ARDS: a secondary analysis of the HARP-2 randomised clinical trial.","authors":"Andrew James Boyle, Peter Ferris, Ian Bradbury, John Conlon, Manu Shankar-Hari, Angela J Rogers, Cecilia M O'Kane, Daniel F McAuley","doi":"10.1186/s13054-022-04025-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Interleukin (IL)-18 is a marker of inflammasome activation, and high baseline plasma IL-18 is associated with increased mortality in patients with sepsis-induced ARDS. The aim of this analysis was to determine if simvastatin was associated with benefit in patients with ARDS and high plasma IL-18.</p><p><strong>Methods: </strong>In this secondary analysis of the HARP-2 study, we compared 28-day mortality and response to simvastatin according to baseline plasma IL-18 using cox proportional hazards analysis. Separately, monocyte-derived macrophages from healthy volunteers were pre-incubated with simvastatin or rosuvastatin before stimulation with ATP and LPS, and the effect on secreted IL-18 and IL-1β compared.</p><p><strong>Results: </strong>511 patients from HARP-2 had available data. High baseline plasma IL-18 (≥ 800 pg/ml) was associated with increased 28-day mortality (high IL-18 30.6% vs. low IL-18 17.5%; HR 1.89 [95% CI 1.30-2.73]; p = 0.001). Allocation to simvastatin in patients with high baseline plasma IL-18 was associated with a lower probability of 28-day mortality compared with placebo (24.0% vs 36.8%; p = 0.01). Finally, simvastatin, but not rosuvastatin, reduced stimulated macrophage secretion of IL-18 and IL-1β.</p><p><strong>Conclusion: </strong>In patients with high baseline plasma IL-18, simvastatin is associated with a higher probability of survival, and this effect may be due to reduced inflammasome activation. These data suggest that baseline plasma IL-18 may allow a personalised treatment approach by identifying patients with ARDS who could benefit from simvastatin therapy.</p>","PeriodicalId":92888,"journal":{"name":"Critical care (Houten, Netherlands)","volume":" ","pages":"164"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9175337/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care (Houten, Netherlands)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13054-022-04025-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Interleukin (IL)-18 is a marker of inflammasome activation, and high baseline plasma IL-18 is associated with increased mortality in patients with sepsis-induced ARDS. The aim of this analysis was to determine if simvastatin was associated with benefit in patients with ARDS and high plasma IL-18.
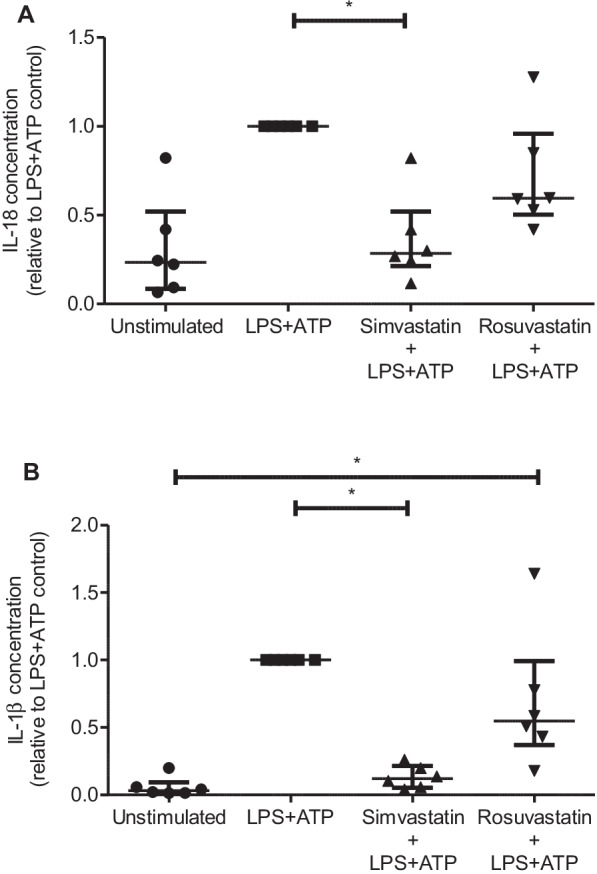
Methods: In this secondary analysis of the HARP-2 study, we compared 28-day mortality and response to simvastatin according to baseline plasma IL-18 using cox proportional hazards analysis. Separately, monocyte-derived macrophages from healthy volunteers were pre-incubated with simvastatin or rosuvastatin before stimulation with ATP and LPS, and the effect on secreted IL-18 and IL-1β compared.
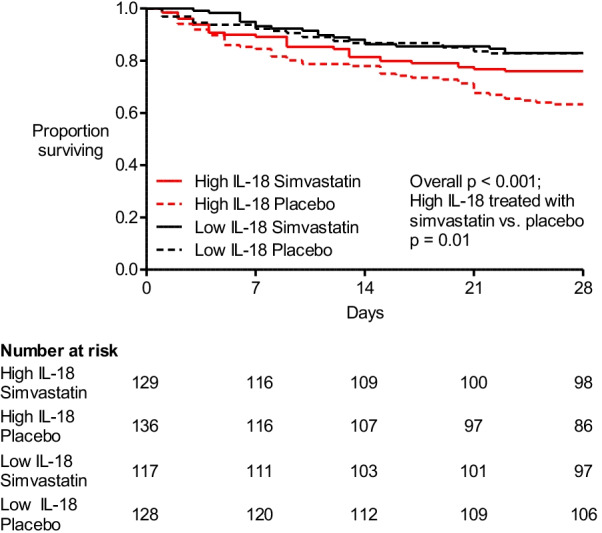
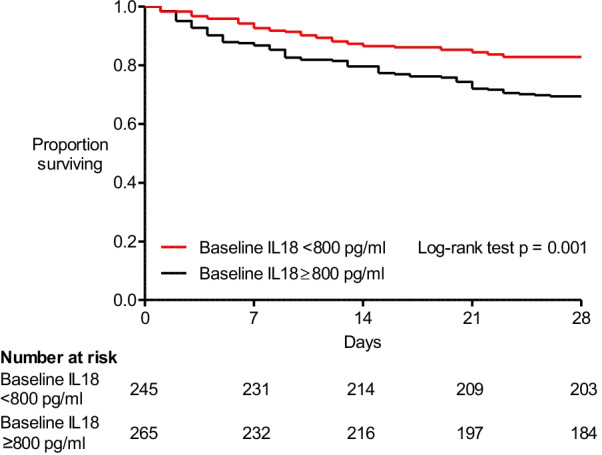
Results: 511 patients from HARP-2 had available data. High baseline plasma IL-18 (≥ 800 pg/ml) was associated with increased 28-day mortality (high IL-18 30.6% vs. low IL-18 17.5%; HR 1.89 [95% CI 1.30-2.73]; p = 0.001). Allocation to simvastatin in patients with high baseline plasma IL-18 was associated with a lower probability of 28-day mortality compared with placebo (24.0% vs 36.8%; p = 0.01). Finally, simvastatin, but not rosuvastatin, reduced stimulated macrophage secretion of IL-18 and IL-1β.
Conclusion: In patients with high baseline plasma IL-18, simvastatin is associated with a higher probability of survival, and this effect may be due to reduced inflammasome activation. These data suggest that baseline plasma IL-18 may allow a personalised treatment approach by identifying patients with ARDS who could benefit from simvastatin therapy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
