J R Younce, R H Cascella, B D Berman, H A Jinnah, S Bellows, J Feuerstein, A Wagle Shukla, A Mahajan, F C F Chang, K R Duque, S Reich, S Pirio Richardson, A Deik, N Stover, J M Luna, S A Norris
{"title":"Anatomical categorization of isolated non-focal dystonia: novel and existing patterns using a data-driven approach.","authors":"J R Younce, R H Cascella, B D Berman, H A Jinnah, S Bellows, J Feuerstein, A Wagle Shukla, A Mahajan, F C F Chang, K R Duque, S Reich, S Pirio Richardson, A Deik, N Stover, J M Luna, S A Norris","doi":"10.3389/dyst.2023.11305","DOIUrl":null,"url":null,"abstract":"<p><p>According to expert consensus, dystonia can be classified as focal, segmental, multifocal, and generalized, based on the affected body distribution. To provide an empirical and data-driven approach to categorizing these distributions, we used a data-driven clustering approach to compare frequency and co-occurrence rates of non-focal dystonia in pre-defined body regions using the Dystonia Coalition (DC) dataset. We analyzed 1,618 participants with isolated non-focal dystonia from the DC database. The analytic approach included construction of frequency tables, variable-wise analysis using hierarchical clustering and independent component analysis (ICA), and case-wise consensus hierarchical clustering to describe associations and clusters for dystonia affecting any combination of eighteen pre-defined body regions. Variable-wise hierarchical clustering demonstrated closest relationships between bilateral upper legs (distance = 0.40), upper and lower face (distance = 0.45), bilateral hands (distance = 0.53), and bilateral feet (distance = 0.53). ICA demonstrated clear grouping for the a) bilateral hands, b) neck, and c) upper and lower face. Case-wise consensus hierarchical clustering at k = 9 identified 3 major clusters. Major clusters consisted primarily of a) cervical dystonia with nearby regions, b) bilateral hand dystonia, and c) cranial dystonia. Our data-driven approach in a large dataset of isolated non-focal dystonia reinforces common segmental patterns in cranial and cervical regions. We observed unexpectedly strong associations between bilateral upper or lower limbs, which suggests that symmetric multifocal patterns may represent a previously underrecognized dystonia subtype.</p>","PeriodicalId":72853,"journal":{"name":"Dystonia","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10621194/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Dystonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/dyst.2023.11305","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/8 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
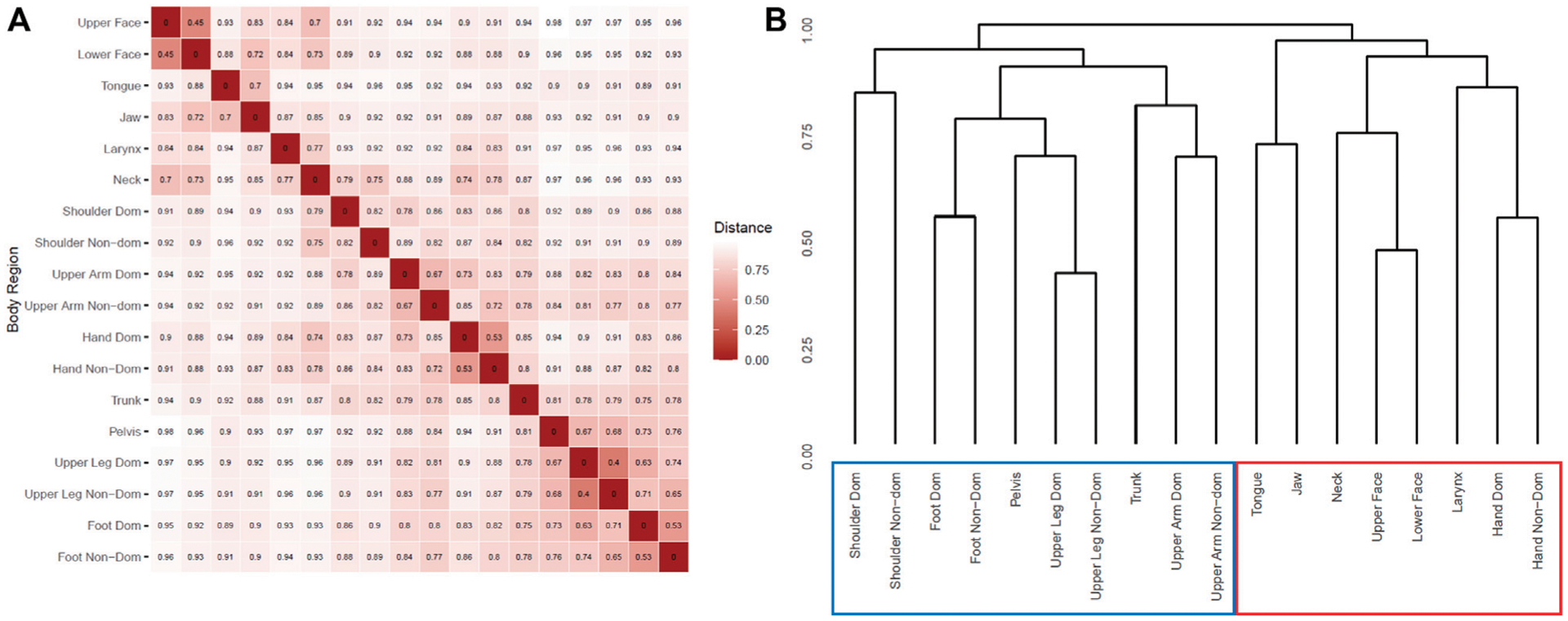
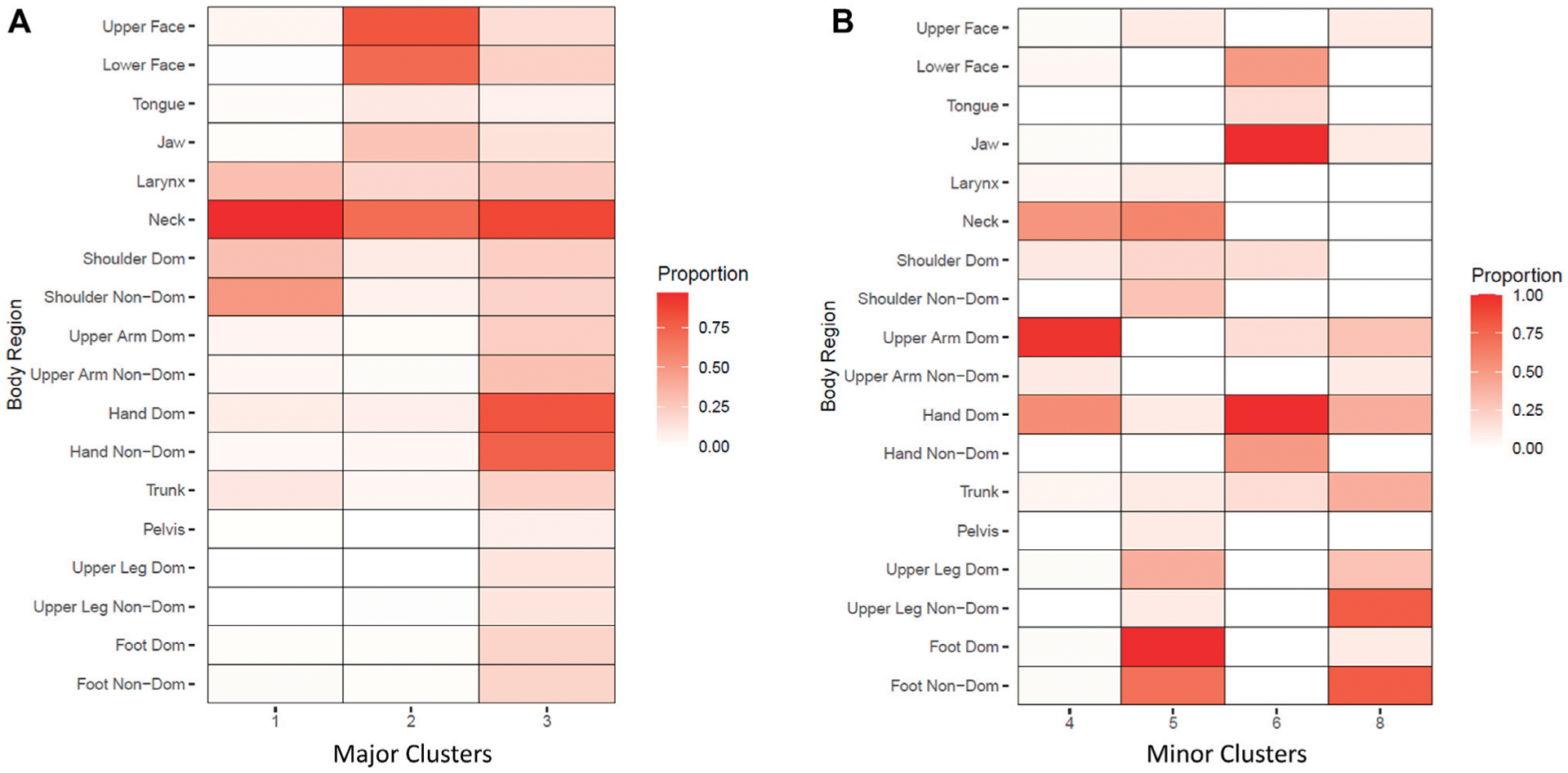
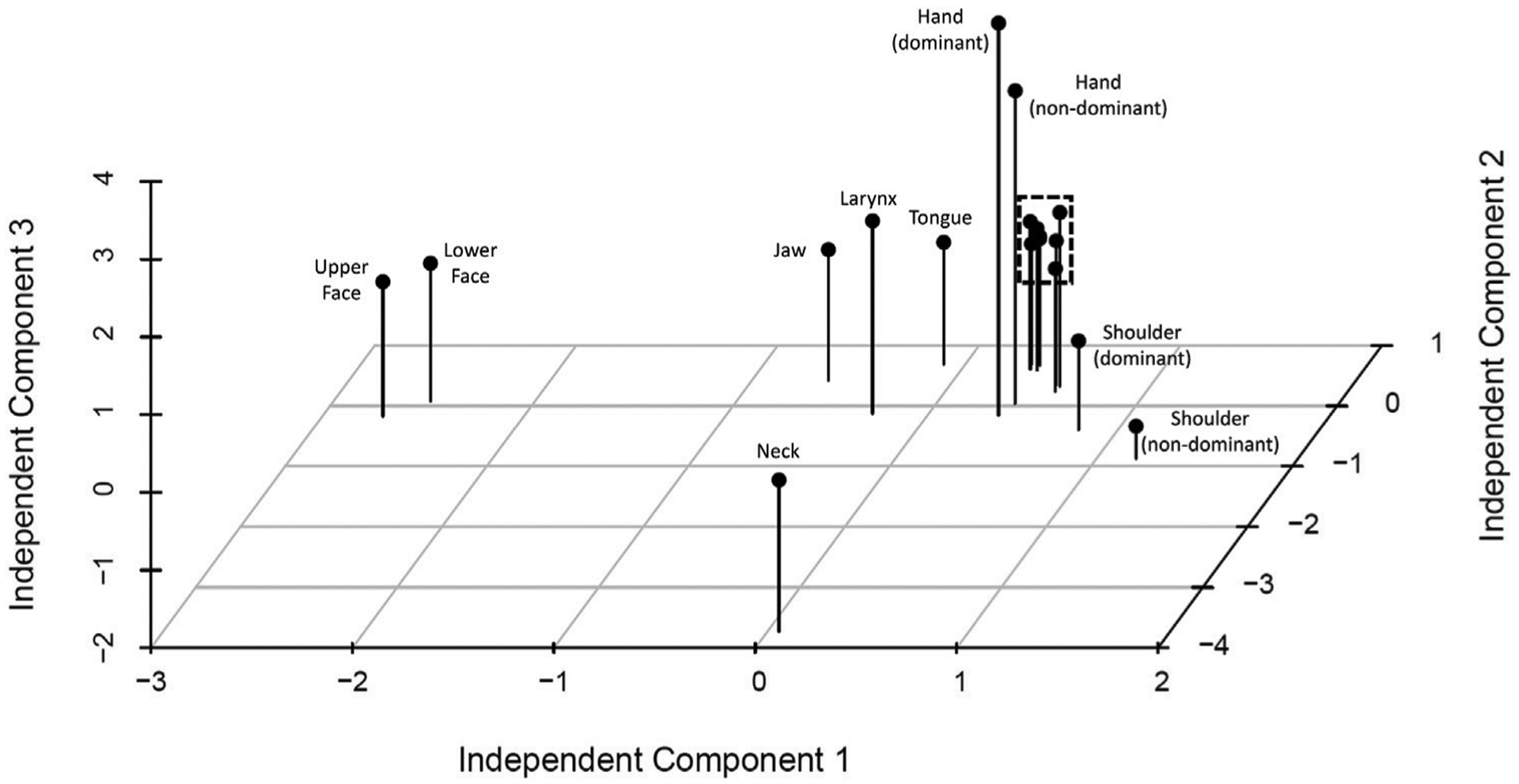
According to expert consensus, dystonia can be classified as focal, segmental, multifocal, and generalized, based on the affected body distribution. To provide an empirical and data-driven approach to categorizing these distributions, we used a data-driven clustering approach to compare frequency and co-occurrence rates of non-focal dystonia in pre-defined body regions using the Dystonia Coalition (DC) dataset. We analyzed 1,618 participants with isolated non-focal dystonia from the DC database. The analytic approach included construction of frequency tables, variable-wise analysis using hierarchical clustering and independent component analysis (ICA), and case-wise consensus hierarchical clustering to describe associations and clusters for dystonia affecting any combination of eighteen pre-defined body regions. Variable-wise hierarchical clustering demonstrated closest relationships between bilateral upper legs (distance = 0.40), upper and lower face (distance = 0.45), bilateral hands (distance = 0.53), and bilateral feet (distance = 0.53). ICA demonstrated clear grouping for the a) bilateral hands, b) neck, and c) upper and lower face. Case-wise consensus hierarchical clustering at k = 9 identified 3 major clusters. Major clusters consisted primarily of a) cervical dystonia with nearby regions, b) bilateral hand dystonia, and c) cranial dystonia. Our data-driven approach in a large dataset of isolated non-focal dystonia reinforces common segmental patterns in cranial and cervical regions. We observed unexpectedly strong associations between bilateral upper or lower limbs, which suggests that symmetric multifocal patterns may represent a previously underrecognized dystonia subtype.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
