{"title":"Subsequent cholecystectomy improve recurrent biliary event-free survival in high-risk acute cholecystitis patients after gallbladder drainage","authors":"Chi-Chih Wang, Chang-Cheng Su, Yen-Pin Huang, Wen-Hsin Huang, Tsung-Yu Tsai, Wen-Wei Sung, Tzu-Wei Yang, Jaw-Town Lin, Chun-Che Lin, Hsu-Heng Yen, Ming-Chang Tsai","doi":"10.1002/aid2.13358","DOIUrl":null,"url":null,"abstract":"<p>Cholelithiasis is a disease with increasing prevalence over the decades. Gallbladder drainage (GBD) is an alternative choice in critically ill patients who cannot tolerate early surgery for acute cholecystitis. In previous data, early or delayed cholecystectomy (CCY) leads to less recurrent biliary events (RBEs) comparing to using a wait-and-see strategy. We wondered if a subsequent CCY strategy after GBD can benefit patients with high surgical risk. This study aimed to explore the clinical outcome after percutaneous transhepatic GBD and risk factors for RBEs. We studied 180 adult acute cholecystitis patients who received percutaneous transhepatic GBD during index admission between July 2017 and December 2018 in Chung Shan Medical University Hospital and Changhua Christian Hospital after exclusion of patients died during the index admission or lost follow-up within 30 days. We further divided these patients into those who received subsequent CCY within 2 months and those who received no CCY within 2 months. RBEs, mortality, and biliary event-related mortality were compared. Multivariate analysis was applied to find the most important factors of RBE-free survival. There were 8 cases (13.6%) in the subsequent CCY group that experienced recurrent biliary events, whereas 39 cases (32.2%) experienced recurrent biliary events in the no CCY within 2 months group. The proportion and average recurrent biliary events per person were all significantly lower in the subsequent CCY group. Although the overall mortality rate was higher in the group that had no CCY within 2 months (16.5% vs 5.1%), the RBE-related mortality difference was insignificant. The most decisive factor to determine RBE-free survival is whether there was a subsequent CCY or not (HR: 0.485, 95% CI: 0.250-0.941, <i>P</i> = .032). We found that subsequent CCY can decrease further RBEs and improve RBE-free survival in high-risk patients with acute cholecystitis that accepted percutaneous transhepatic GBD initially.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"11 1","pages":"33-40"},"PeriodicalIF":0.4000,"publicationDate":"2022-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13358","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13358","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
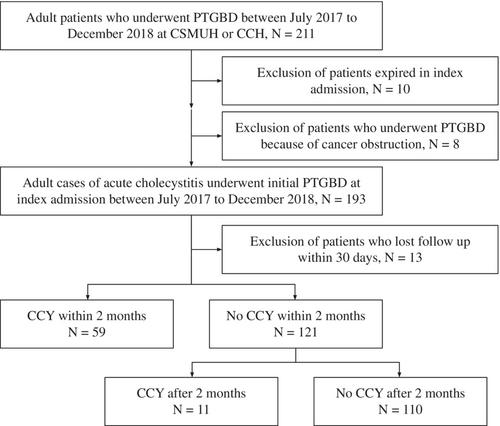
Cholelithiasis is a disease with increasing prevalence over the decades. Gallbladder drainage (GBD) is an alternative choice in critically ill patients who cannot tolerate early surgery for acute cholecystitis. In previous data, early or delayed cholecystectomy (CCY) leads to less recurrent biliary events (RBEs) comparing to using a wait-and-see strategy. We wondered if a subsequent CCY strategy after GBD can benefit patients with high surgical risk. This study aimed to explore the clinical outcome after percutaneous transhepatic GBD and risk factors for RBEs. We studied 180 adult acute cholecystitis patients who received percutaneous transhepatic GBD during index admission between July 2017 and December 2018 in Chung Shan Medical University Hospital and Changhua Christian Hospital after exclusion of patients died during the index admission or lost follow-up within 30 days. We further divided these patients into those who received subsequent CCY within 2 months and those who received no CCY within 2 months. RBEs, mortality, and biliary event-related mortality were compared. Multivariate analysis was applied to find the most important factors of RBE-free survival. There were 8 cases (13.6%) in the subsequent CCY group that experienced recurrent biliary events, whereas 39 cases (32.2%) experienced recurrent biliary events in the no CCY within 2 months group. The proportion and average recurrent biliary events per person were all significantly lower in the subsequent CCY group. Although the overall mortality rate was higher in the group that had no CCY within 2 months (16.5% vs 5.1%), the RBE-related mortality difference was insignificant. The most decisive factor to determine RBE-free survival is whether there was a subsequent CCY or not (HR: 0.485, 95% CI: 0.250-0.941, P = .032). We found that subsequent CCY can decrease further RBEs and improve RBE-free survival in high-risk patients with acute cholecystitis that accepted percutaneous transhepatic GBD initially.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
