Yingren Mai, Zhiyu Cao, Lei Zhao, Qun Yu, Jiaxin Xu, Wenyan Liu, Bowen Liu, Jingyi Tang, Yishan Luo, Wang Liao, Wenli Fang, Yuting Ruan, Ming Lei, Vincent C. T. Mok, Lin Shi, Jun Liu, for the Alzheimer's Disease Neuroimaging Initiative
{"title":"The role of visual rating and automated brain volumetry in early detection and differential diagnosis of Alzheimer's disease","authors":"Yingren Mai, Zhiyu Cao, Lei Zhao, Qun Yu, Jiaxin Xu, Wenyan Liu, Bowen Liu, Jingyi Tang, Yishan Luo, Wang Liao, Wenli Fang, Yuting Ruan, Ming Lei, Vincent C. T. Mok, Lin Shi, Jun Liu, for the Alzheimer's Disease Neuroimaging Initiative","doi":"10.1111/cns.14492","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Medial temporal lobe atrophy (MTA) is a diagnostic marker for mild cognitive impairment (MCI) and Alzheimer's disease (AD), but the accuracy of quantitative MTA (QMTA) in diagnosing early AD is unclear. This study aimed to investigate the accuracy of QMTA and its related components (inferior lateral ventricle [ILV] and hippocampus) with MTA in the early diagnosis of MCI and AD.</p>\n </section>\n \n <section>\n \n <h3> Method<b>s</b></h3>\n \n <p>This study included four groups: normal (NC), MCI stable (MCIs), MCI converted to AD (MCIs), and mild AD (M-AD) groups. Magnetic resonance image analysis software was used to quantify the hippocampus, ILV, and QMTA. MTA was rated by two experienced neurologists. Receiver operating characteristic area under the curve (AUC) analysis was performed to compare their capability in differentiating AD from NC and MCI, and optimal thresholds were determined using the Youden index.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>QMTA distinguished M-AD from NC and MCI with higher diagnostic accuracy than MTA, hippocampus, and ILV (AUC<sub>NC</sub> = 0.976, AUC<sub>MCI</sub> = 0.836, AUC<sub>MCIs</sub> = 0.894, AUC<sub>MCIc</sub> = 0.730). The diagnostic accuracy of QMTA was superior to that of MTA, the hippocampus, and ILV in differentiating MCI from AD. The diagnostic accuracy of QMTA was found to remain the best across age, sex, and pathological subgroups analyzed. The sensitivity (92.45%) and specificity (90.64%) were higher in this study when a cutoff value of 0.635 was chosen for QMTA.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>QMTA may be a better choice than the MTA scale or the associated quantitative components alone in identifying AD patients and MCI individuals with higher progression risk.</p>\n </section>\n </div>","PeriodicalId":154,"journal":{"name":"CNS Neuroscience & Therapeutics","volume":"30 4","pages":""},"PeriodicalIF":5.0000,"publicationDate":"2023-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cns.14492","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CNS Neuroscience & Therapeutics","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cns.14492","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
Background
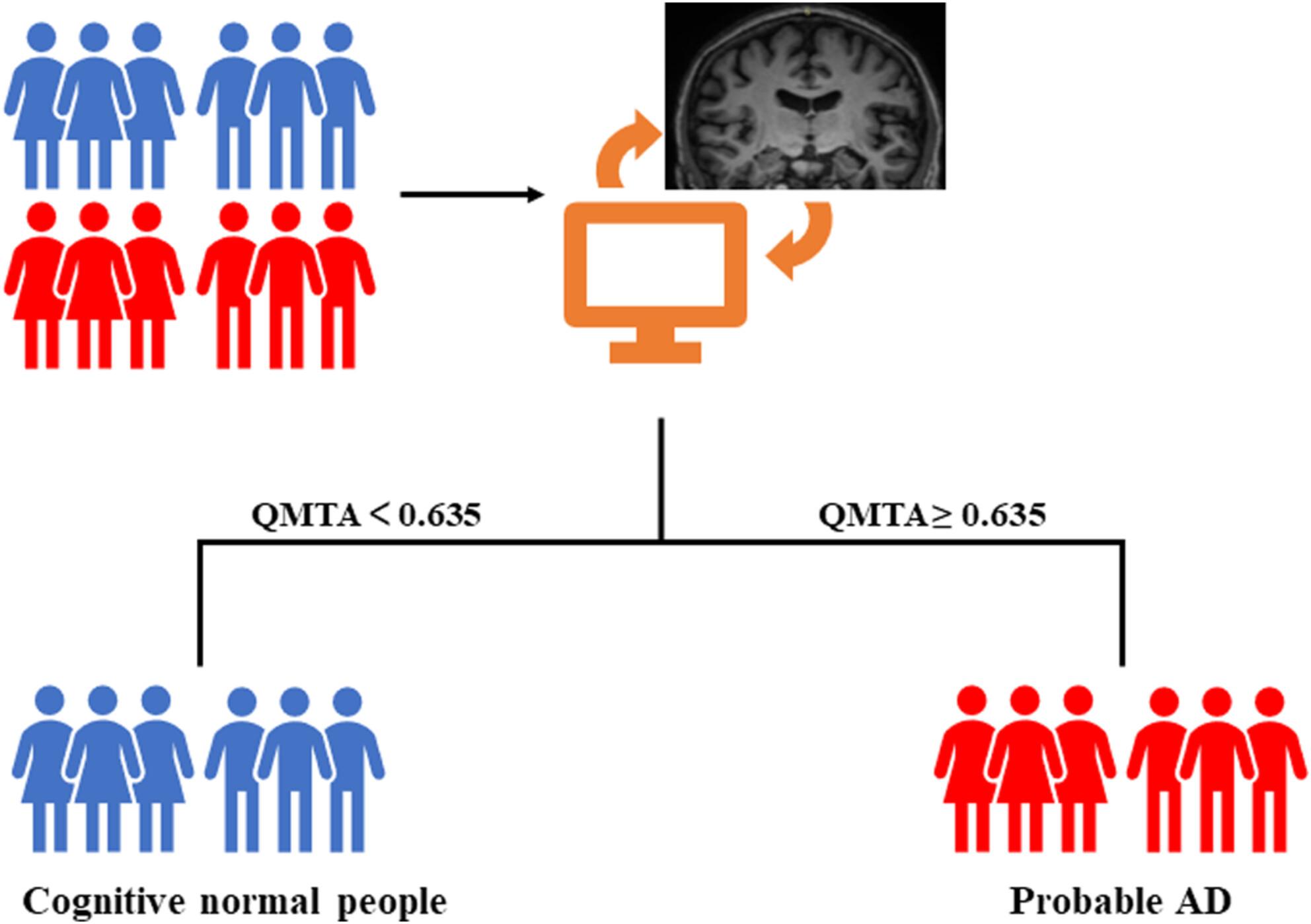
Medial temporal lobe atrophy (MTA) is a diagnostic marker for mild cognitive impairment (MCI) and Alzheimer's disease (AD), but the accuracy of quantitative MTA (QMTA) in diagnosing early AD is unclear. This study aimed to investigate the accuracy of QMTA and its related components (inferior lateral ventricle [ILV] and hippocampus) with MTA in the early diagnosis of MCI and AD.
Methods
This study included four groups: normal (NC), MCI stable (MCIs), MCI converted to AD (MCIs), and mild AD (M-AD) groups. Magnetic resonance image analysis software was used to quantify the hippocampus, ILV, and QMTA. MTA was rated by two experienced neurologists. Receiver operating characteristic area under the curve (AUC) analysis was performed to compare their capability in differentiating AD from NC and MCI, and optimal thresholds were determined using the Youden index.
Results
QMTA distinguished M-AD from NC and MCI with higher diagnostic accuracy than MTA, hippocampus, and ILV (AUCNC = 0.976, AUCMCI = 0.836, AUCMCIs = 0.894, AUCMCIc = 0.730). The diagnostic accuracy of QMTA was superior to that of MTA, the hippocampus, and ILV in differentiating MCI from AD. The diagnostic accuracy of QMTA was found to remain the best across age, sex, and pathological subgroups analyzed. The sensitivity (92.45%) and specificity (90.64%) were higher in this study when a cutoff value of 0.635 was chosen for QMTA.
Conclusions
QMTA may be a better choice than the MTA scale or the associated quantitative components alone in identifying AD patients and MCI individuals with higher progression risk.
期刊介绍:
CNS Neuroscience & Therapeutics provides a medium for rapid publication of original clinical, experimental, and translational research papers, timely reviews and reports of novel findings of therapeutic relevance to the central nervous system, as well as papers related to clinical pharmacology, drug development and novel methodologies for drug evaluation. The journal focuses on neurological and psychiatric diseases such as stroke, Parkinson’s disease, Alzheimer’s disease, depression, schizophrenia, epilepsy, and drug abuse.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
